Introduction
The use of self-etch primers has increased steadily because of their time savings and greater simplicity; however, overall benefits and potential disadvantages and harms have not been assessed systematically. In this study, we reviewed randomized controlled trials to assess the risk of attachment failure, bonding time, and demineralization adjacent to attachments between 1-stage (self-etch) and 2-stage (acid etch) bonding in orthodontic patients over a minimum follow-up period of 12 months.
Methods
Data sources were electronic databases including MEDLINE, EMBASE, the Cochrane Oral Health Group’s Trials Register, and CENTRAL, without language restrictions. Unpublished literature was searched on ClinicalTrials.gov , the National Research Register, and Pro-Quest Dissertation Abstracts and Thesis database. Authors were contacted when necessary, and reference lists of the included studies were screened. Search terms included randomized controlled trial, controlled clinical trial, random allocation, double-blind method, single-blind method, orthodontics, self-etch, SEP, primer, and bonding agent. Randomized clinical trials directly comparing self-etch and acid-etch primers with respect to the predefined outcomes and including patients with full-arch, fixed, and bonded orthodontic appliances (not banded) with follow-up periods of at least 12 months were included. Using predefined forms, 2 authors undertook independent data extraction with conflict resolution by the third author. Randomized clinical trial quality assessment based on the Cochrane Risk of Bias tool was also used.
Results
Eleven studies met the inclusion criteria; 6 were excluded because of a high risk of bias. In total, 1721 brackets bonded with acid-etch and 1723 with self-etch primer techniques were included in the quantitative synthesis. Relatively low statistical and clinical heterogeneity was observed among the 5 randomized clinical trials (n = 3444 brackets) comparing acid-etch with self-etch primers. A random effects meta-analysis demonstrated a tendency for a higher risk of failure (odds ratio, 1.35; 95% CI, 0.99-1.83; P = 0.06) with self-etch primers. A small but statistically significant time saving was also associated with the self-etch primer technique (weighted mean difference, 23.2 seconds per bracket; 95% CI, 20.7-25.8; P <0.001). There was insufficient evidence to assess the effect of bonding modality on demineralization rates.
Conclusions
There is weak evidence indicating higher odds of failure with self-etch primer than acid etch over 12 months in orthodontic patients, and there is strong evidence that a self-etch primer is likely to result in a modest time savings (8 minutes for full bonding) compared with acid etch.
Dental bonding was introduced by Bowen after the pioneering work on enamel preparation techniques of Buonocore et al. These principles were subsequently applied to orthodontics, revolutionizing appliances physically and cosmetically, with multi-banded systems becoming obsolete and superseded by bonded appliances.
Further progress has been made in relation to bonding with an emphasis on streamlining the process, enhancing performance in a moist environment, and improving resistance to demineralization. In recent years, there has been growing interest in 1-step bonding systems, which do not rely on separate application of etchant and bonding material. Self-etch bonding systems or self-etch primers (SEPs) are routinely used by 29.5% of practitioners in the United States. These systems typically incorporate methacrylated phosphoric acid esters; after application to enamel, the phosphate group dissolves and removes calcium ions from hydroxyapatite, becoming incorporated in the network before the primer polymerizes, neutralizing the acid.
The proposed advantages of SEPs include reduced chair-side time, although this is tempered by the requirement for judicious pumicing before bonding procedures to minimize the risk of failure ; reduced sensitivity to moisture; and reduced inventory requirements. However, although the performance of SEPs has been compared with conventional acid-etch (AE) techniques in randomized controlled trials, a comparison of these techniques in the context of a systematic review has not been undertaken. The aims of this study were therefore to compare 1-step and 2-step bonding procedures with respect to attachment failure rates and time taken to place attachments.
Material and methods
The protocol for a systematic review of SEPs was registered on the National Institute of Health Research Database ( www.crd.york.ac.uk/prospero , Protocol: CRD42011001601). The following selection criteria were applied for the review.
- 1.
Study design: randomized and controlled clinical trials, with split-mouth designs included.
- 2.
Participants: patients with full-arch, fixed, and bonded orthodontic appliances.
- 3.
Interventions: SEPs were used to prepare tooth surfaces before bonding the orthodontic attachments in the intervention sample. The control group’s appliances were bonded with the conventional, 2-step AE technique.
- 4.
Exclusion criteria: studies using banded attachments and those involving follow-up periods of less than 12 months were omitted from the review.
- 5.
Outcome measures: the main outcome measure was first-time bond failure with both bonding systems. Secondary outcome measures included time required to place individual brackets and decalcification. The attachment failures with each enamel preparation technique were recorded. When available, the time taken for failures to occur was also recorded. The time taken to place attachments with each technique and the presence of demineralization adjacent to the bonded attachments were noted, in addition to the severity of each lesion.
The following electronic databases were searched: MEDLINE (1966 to July 2011; Appendix ), EMBASE (1980 to July 2011), Cochrane Oral Health Group’s Trials Register (March 2011), Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library Issue 2, 2011). Language restrictions were not applied. Unpublished literature was searched electronically by using ClinicalTrials.gov ( www.clinicaltrials.gov ) and the National Research Register ( www.controlled-trials.com ) with the term “orthodontic” and “bond.” In addition, the Pro-Quest Dissertation Abstracts and Thesis database was searched ( www.lib.umi.com./dissertations ) by using “orthodontic*” and “bond*.” Conference proceedings and abstracts were also accessed when possible. Authors were contacted to identify unpublished or ongoing clinical trials and to clarify data as required. Reference lists of the included studies were screened for relevant research.
Assessment of research for inclusion in the review, assessment of risk of bias, and extraction of data were performed independently and in duplicate by 2 investigators (P.S.F. and A.J.) who were not blinded to the authors or the results of the research. Disagreements were resolved by discussion and consultation with the third author (N.P.).
Seven criteria were analyzed to grade the risk of bias inherent in each study, including random sequence generation, allocation concealment, blinding of participants and personnel, blinding of assessors, incomplete outcome data, selective reporting of outcomes, and other potential sources of bias. An overall assessment of risk of bias (high, unclear, low) was made for each included trial by using the Cochrane Collaboration risk of bias tool. Studies with at least 1 criterion designated to be at high risk of bias were regarded as having a high risk of bias overall and excluded from the meta-analysis.
A data extraction form was developed to record study design, observation period, participants, interventions, outcomes, and outcome data of interest, including risk of failure of attachments, time taken to place attachments, and severity of demineralization when applicable. Clinical heterogeneity of the included studies was gauged by assessing the treatment protocol—particularly, participants and settings, materials used, timing of data collection, and measurement techniques. Statistical heterogeneity was assessed by inspecting a graphic display of the estimated treatment effects from the trials in conjunction with 95% confidence intervals. The chi-square test was used to assess for heterogeneity; a P value below 0.1 meant significant heterogeneity. I 2 tests for homogeneity were undertaken to quantify the extent of heterogeneity before each meta-analysis. I 2 values above 50% would signify moderate to high heterogeneity and might preclude meta-analysis. A weighted treatment effect was calculated, and the results for attachment failure were expressed as odds ratios. For time required to place attachments, mean differences with 95% confidence intervals were calculated for each trial and combined by using a random-effects model, which was considered more appropriate in view of the variations in populations and settings. For continuous outcomes, mean differences and standard errors were entered for parallel and split-mouth designs. When necessary, standard errors for the split-mouth designs were calculated. If more than 10 studies were included in the meta-analysis, standard funnel plots and contoured enhanced funnel plots would be drawn to identify publication bias.
Statistical analysis
Sensitivity analyses were prespecified to deal with studies at higher risk of bias, publication bias, and other potential sources of heterogeneity including dominant effects of at least 1 large study and differences in outcome related to specific SEPs to isolate their influence on the overall outcome. Meta-analyses and sensitivity analyses were undertaken using the Stata statistical software package (version 12.1; StataCorp, College Station, Tex) by using “metan” and “metainf” commands.
Results
Forty-eight trials were initially deemed potentially relevant to the review ( Fig 1 ). After we reviewed the abstracts, initially 13 satisfied the inclusion criteria. Two of these were subsequently excluded after retrieval of the full-text article because of duplicate publication of the data and comparison of 2 SEPs without a control group involving conventional etch preparation.
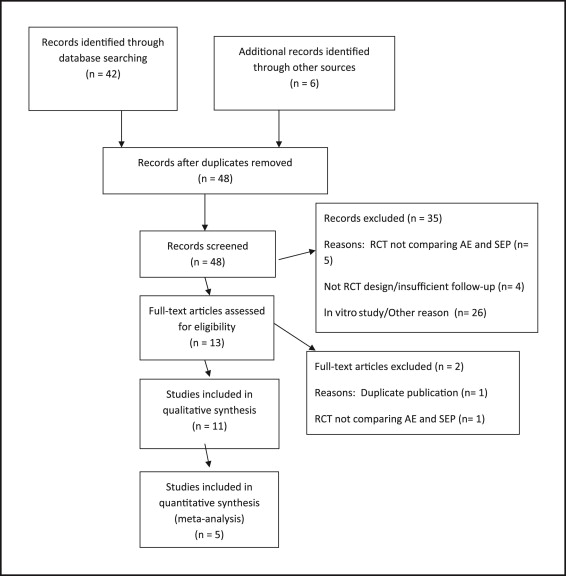
Of the final 11 articles included in the qualitative analysis, all were prospective clinical trials ( Tables I and II ). Although all of these were variously described as randomized controlled trials, the randomization procedure was considered inadequate in 5 studies. Consequently, allocation concealment was likely to have been subverted, thus increasing the risk of bias. These studies were excluded from the quantitative synthesis ( Tables III and IV ). Of the remaining studies, 4 were split-mouth designs, and 2 were parallel-group randomized controlled trials.
| Study | Method | Observation period | Participants | Interventions | Outcome |
|---|---|---|---|---|---|
| Aljubouri et al (2004) | Split-mouth RCT | 6 and 12 months | 51 participants: 16 male, 35 female 32 <15 years, 19 >15 years |
389 brackets bonded with SEP, 388 bonded with AE (353 paired per group) | Bond failure risk Bonding time |
| Manning et al (2006) | Parallel-group RCT | 6 and 12 months; overall treatment | 34 participants, 17 per group: 11 male, 23 female. Ages, 11-16 years | 299 brackets bonded with SEP and 298 with AE | Bond failure risk |
| House et al (2006) | Split-mouth RCT | 1, 6, and 12 months | 30 participants: only 20 were analyzed because trial stopped prematurely | 339 brackets bonded with Ideal 1 SEP and AE | Bond failure risk |
| Murfitt et al (2006) | Split-mouth RCT | 12 months | 39 participants: 13 male, 26 female. Mean age, 14.4 (SD, 2.5) years | 661 brackets bonded overall with SEP (331) and AE (330) | Bond failure risk |
| Banks and Thiruvenkatachari (2008) | Parallel-group RCT | Overall treatment | 60 participants, 30 per group: 23 male, 37 female. Ages, 11-18 years | 30 participants (438 brackets) with TransBond Plus SEP; 30 participants (433 brackets) with AE | Bond failure risk |
| Cal-Neto et al (2009) | Parallel-group RCT | 12 months | 28 participants, 14 per group: Mean age, 14.92 years; 11 male, 17 female | 276 brackets bonded with SEP and 272 brackets with AE | Bond failure risk |
| Study | Method | Observation periods | Participants | Interventions | Outcome |
|---|---|---|---|---|---|
| Pandis et al (2006) | Split-mouth RCT | 12 months | 62 participants: 23 male, 39 female. Mean age, 14 years | 610 brackets bonded with TransBond Plus SEP, 610 bonded with AE and OrthoSolo primer | Bond failure risk |
| Pandis et al (2006) | Split-mouth RCT | 15 months | 62 participants: 23 male, 39 female. Mean age, 13.7 years | 221 molar tubes bonded with TransBond Plus SEP, 223 molar tubes bonded with AE and OrthoSolo primer | Bond failure risk |
| Reis et al (2008) | Split-mouth RCT | 18 months | 30 participants: 15 male, 15 female. Ages, 12-18 years | 283 brackets bonded with SEP and 283 with AE | Bond failure risk |
| Elekdag-Turk et al (2008) | Split-mouth RCT | 6 and 12 months | 39 participants: 23 male, 39 female. Mean age, 15.58 years | 344 brackets bonded with SEP and 344 with AE | Bond failure risk |
| Ghiz et al (2009) | Split-mouth RCT | 18 to 24 months | 25 participants. No demographics given | 236 brackets bonded with SEP and 233 brackets with AE | Demineralization |
| Trial | Random sequence generation | Allocation concealment | Blinding participants and personnel | Blinding assessor | Free of incomplete outcome data | Free of selective reporting | Free of other threats to validity |
|---|---|---|---|---|---|---|---|
| Aljubouri et al (2004) | Low | Low | Unclear | Unclear | Low | Low | Low |
| Manning et al (2006) | Low | Unclear | Unclear | Unclear | Low | Low | Low |
| House et al (2006) | Low | Low | Low | Unclear | Low | Low | High |
| Murfitt et al (2006) | Low | Low | Low | Unclear | Low | Low | Low |
| Banks and Thirvenkatachari (2008) | Low | Low | Low | Unclear | Low | Low | Low |
| Cal-Neto et al (2009) | Low | Low | Unclear | Unclear | Low | Low | Low |
| Trial | Random sequence generation | Allocation concealment | Blinding participants and personnel | Blinding assessor | Free of incomplete outcome data | Free of selective reporting | Free of other threats to validity |
|---|---|---|---|---|---|---|---|
| Pandis et al (2006) | High | High | Unclear | Unclear | Low | Low | Low |
| Pandis et al (2006) | High | High | Unclear | Unclear | Low | Low | Low |
| Reis et al (2008) | High | High | Unclear | Unclear | Low | Low | Low |
| Elekdag-Turk et al (2008) | High | High | Unclear | Unclear | Low | Low | Low |
| Ghiz et al (2009) | High | High | Unclear | Unclear | Low | Low | Low |
Of the 7 criteria used to assess risk of bias, similar results were obtained throughout for 3 criteria: completeness of data reporting, absence of selective reporting, and blinding of assessors. In particular, complete outcome data were reported in all studies without selective reporting of results ( Tables III and IV ; Fig 2 ). Additionally, blinding of assessors was considered unlikely, since the researchers themselves were involved in placing the appliances, precluding blinding. Blinding of assessors was not mentioned in any reports. Nevertheless, some authors explicitly mentioned attempts to blind the participants to the mode of bonding, although this is likely to pertain equally to all split-mouth studies. Nevertheless, the binary primary outcome (bracket failure) was not easily open to manipulation, limiting the potential problems of lack of blinding.
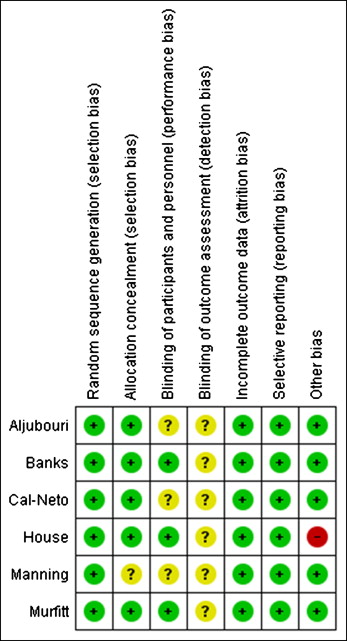
Generation of the random sequence was considered adequate in 6 studies ; allocation concealment was also thought to be reliable in 5 of these studies. The randomization procedure was considered inadequate or not sufficiently clear in the remaining studies. However, each of these studies was split-mouth in design, which might have negated the importance of the randomization procedure. Nevertheless, it was agreed that these trials should be omitted from the quantitative analysis.
Therefore, overall, 6 studies were deemed to be at low or unclear risk of bias and were initially considered appropriate for quantitative synthesis. Early cessation was reported in 1 study because of an unacceptable number of failures with the SEP, causing a threat to validity. Therefore, after further appraisal and discussion, it was decided to omit this study because of the discordant findings resulting in a premature end to the trial related to the excessive failure rates of up to 72%.
The failure risk of attachments was assessed in all 5 included studies. In total, 1721 brackets bonded with AE and 1723 bonded with SEP techniques were included in the quantitative synthesis ( Table V ). Of these, 4.5% (77 brackets) and 6.0% (104 brackets) failed with the AE and the SEP preparation techniques, respectively. The random-effects model assumes that there are different bond failure risks in different settings; the calculated estimate therefore indicates the average effect. Meta-analysis of these studies suggested higher odds of bond failures with the SEP technique, although the difference failed to reach statistical significance ( Table VI ; Fig 3 ; odds ratio, 1.35; 95% CI, 0.99-1.83). The pooled odds ratio from the random-effects model indicated that the failure risk was 35% higher in the SEP group than in the AE group. The 95% confidence interval indicates that the mean effect size can range from 1% to 83% in the SEP group compared with the AE group, verging on statistical significance ( P = 0.06). Based on the heterogeneity of the included studies, the prediction intervals indicate that the true effect size is likely to range from 0.82 to 2.22. The prediction interval was wider than the 95% confidence interval and includes the value 1, indicating that in certain settings no difference is expected in bond failures with the protocols. The test for homogeneity confirmed that meta-analysis of this outcome among the 5 studies was reasonable (I 2 , 0.0%; chi-square, P = 0.497; τ 2 = 0.00).
| Study | Intervention (number of attachments) | Bond failures (%) | Time (s) | ||
|---|---|---|---|---|---|
| AE | SEP | AE | SEP | ||
| Aljubouri et al (2004) | SEP (389), AE (388): 353 paired per group reducing to 312 at 12 months | 11 (3.1) | 6 (1.6) | Mean, 106.6 Mean difference, 24.9 (95% CI, 22.1-27.7) |
Mean, 81.7 |
| Manning et al (2006) | SEP (299), AE (298) | 22 (7.4) | 21 (7) | ||
| House et al (2006) | Ideal 1 SEP (339), AE (339) | 25 (14.8) | 123 (72.4) | ||
| Murfitt et al (2006) | SEP (331), AE (330) | 13 (3.9) | 37 (11.2) | ||
| Banks and Thiruvenkatachari (2008) | SEP 30 participants (438), AE 30 participants (433) | 15 (3.5) | 21 (4.8) | 97.7 (SD, 9.1; 95% CI, 94.3-101.2) | 75.5 (SD, 6.7; 95% CI, 72.9-78.5) |
| Cal-Neto et al (2009) | SEP (276), AE (272) | 13 (4.8) | 19 (6.9) | ||
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


