The aim of this article is to report the clinical orthodontic treatment of an adult patient with 2 impacted maxillary canines. Traction was applied to the impacted teeth; however, after 7 months, the teeth were found to be ankylosed and were extracted. The extraction spaces were closed by moving the posterior teeth mesially with mini-implant anchorage. The results were satisfactory, with the premolars in the functional position of the canines.
The maxillary canines are important teeth in terms of esthetics and function. The likelihood of their failing to erupt or becoming impacted is between 1% and 3%. The causes of canine impaction can be correlated with other dental anomalies and could be due to local factors or a polygenetic, multifactorial inheritance. Local factors are tooth size-arch length discrepancies, prolonged retention or early loss of the deciduous canine, abnormal tooth bud position, alveolar cleft, dilaceration of the root, and idiopathic conditions with no apparent cause. This problem has several solutions.
The impacted tooth could be extracted, autotransplantation could be performed, or the tooth could be surgically exposed and orthodontically moved to another position in the dental arch. The timing of orthodontic treatment, the type of surgical procedure to expose the impacted tooth, the necessary orthodontic mechanics, and potential problems with treatment vary, depending on which tooth is impacted and its position in the jaw.
The objective of this case report is to describe the treatment of an adult with 2 impacted maxillary canines, which were diagnosed as ankylosed after the attempt to erupt them failed. This required extraction of the canines and orthodontic closure of the extraction spaces.
Diagnosis and etiology
At the initial examination, the patient was aged 25 years 5 months and in a good state of general health. She was referred to the orthodontist for orthodontic treatment by her general dentist, who found the 2 impacted maxillary canines ( Fig 1 ).

The patient had an Angle Class I malocclusion and an arch length discrepancy of –8.5 mm in the mandibular arch. Both maxillary canines were impacted, and the mandibular incisors were retroclined (1.NB, 16°). There were normal overlap and overbite, and quadrangular-shaped arches, with symmetry in the anteroposterior and transverse directions ( Figs 1 and 2 ).
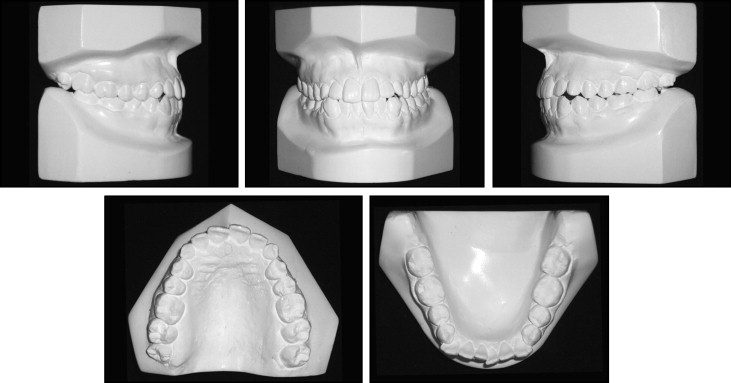
Radiographically, the impaction of the maxillary canines and mandibular third molars could be observed ( Fig 3 ). The cephalometric radiograph showed a small skeletal disharmony in the sagittal direction, with an ANB angle equal to 0° (SNA, 84°; SNB, 84°). This showed a tendency for a skeletal Class III relationship. In the vertical plane of space, all cephalometric measurements indicated a well-balanced face (Go Gn-Sn, 30°; y-axis, 62°; FMA, 30°) ( Figs 3 and 4 ).
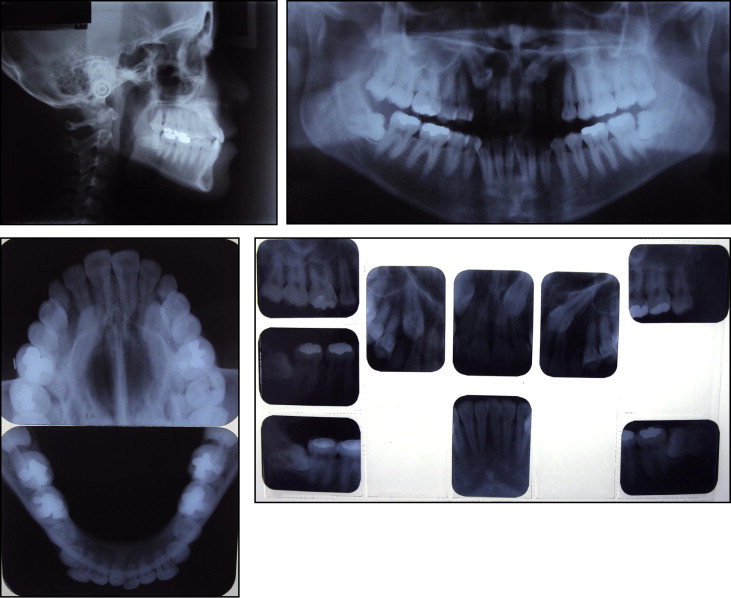
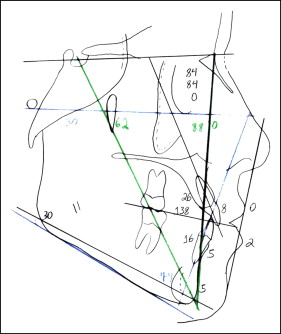
The facial analysis showed a balanced and harmonious face, with lip seal at rest, a straight profile with a slight protrusion of the bottom lip (top lip, S-line, 0 mm; bottom lip, S-line, 2 mm) and an acceptable nasolabial angle ( Figs 1 and 4 ).
Treatment objectives
- 1.
Maxilla: maintain the vertical, anteroposterior, and transverse positions.
- 2.
Mandible: maintain the maxillomandibular relationship during orthodontic treatment.
- 3.
Maxillary teeth: extract the deciduous canines and attempt traction of the impacted permanent canines. If the canines respond well to traction, it would be necessary to extract the first premolars. If the canines are ankylosed, they would be replaced by the first premolars.
- 4.
Mandibular teeth: extract the first premolars to obtain space for alignment and leveling of the canines and the incisors. Maintain the retroclination of the incisors during treatment (1.NB, 16°).
- 5.
Occlusion: establish proper canine occlusion, correct the mandibular crowding, obtain simultaneous bilateral contacts in harmony with centric relation, and disclude the posterior teeth in mandibular excursive movements.
- 6.
Facial esthetics: in conjunction with the patient’s desires, the option was for treatment with extractions instead of orthognathic surgery, knowing the possibility of flattening the facial profile.
Treatment objectives
- 1.
Maxilla: maintain the vertical, anteroposterior, and transverse positions.
- 2.
Mandible: maintain the maxillomandibular relationship during orthodontic treatment.
- 3.
Maxillary teeth: extract the deciduous canines and attempt traction of the impacted permanent canines. If the canines respond well to traction, it would be necessary to extract the first premolars. If the canines are ankylosed, they would be replaced by the first premolars.
- 4.
Mandibular teeth: extract the first premolars to obtain space for alignment and leveling of the canines and the incisors. Maintain the retroclination of the incisors during treatment (1.NB, 16°).
- 5.
Occlusion: establish proper canine occlusion, correct the mandibular crowding, obtain simultaneous bilateral contacts in harmony with centric relation, and disclude the posterior teeth in mandibular excursive movements.
- 6.
Facial esthetics: in conjunction with the patient’s desires, the option was for treatment with extractions instead of orthognathic surgery, knowing the possibility of flattening the facial profile.
Treatment alternatives
- 1.
Orthosurgical treatment, with extraction of the maxillary first premolars to achieve better positioning of the maxillary incisors in addition to eruption and proper positioning of the maxillary canines.
- 2.
Orthodontic treatment with extraction of the 4 first premolars and orthodontic repositioning of the maxillary canines.
- 3.
Attempt traction of the maxillary left and right canines and maintain the maxillary left and right first premolars, without initially extracting them. If the canines responded to treatment favorably, the premolars would be extracted.
- 4.
Treatment associated with extraction of all 4 first premolars.
Treatment progress
The patient declined orthognathic surgery because she had no esthetic complaints regarding her face. Therefore, in conjunction with the patient, we decided to extract the 4 first premolars. The patient was informed with respect to the possible ankylosis of the maxillary canines and also that attempts to move them would lead to an increased treatment time. In the maxillary arch, initially only the deciduous canines were extracted, because if traction of the permanent canines was unsuccessful, the first premolars could replace them.
The plan was to place fixed orthodontic appliances in the maxillary and mandibular dental arches by using conventional edgewise brackets with 0.022 × 0.028-in slots, except for the mandibular incisors, which initially were not moved until there was space for aligning and leveling after partial retraction of the canines.
In the maxillary arch, stainless steel archwires, from 0.014 to 0.020 in, were used for alignment and leveling. After this, the maxillary deciduous canines were extracted, and surgical uncovering of the permanent canines was performed. A stainless steel arch was made of a rectangular section of 0.019 × 0.025-in archwire, with first- and third-order bends. Helical springs were welded between the lateral incisors and the first premolars, and a force of 100 g was applied to the canines ( Fig 5 ). After 7 months of traction, opening of the bite in the incisor region was verified radiographically ( Fig 6 ), and the canines were in the same position ( Fig 7 ). Therefore, extraction of these teeth was requested, and the first premolars were used to replace them.


