Salivary diagnostics is a dynamic and emerging field utilizing nanotechnology and molecular diagnostics to aid in the diagnosis of oral and systemic diseases. In this article the author critically reviews the latest advances using oral biomarkers for disease detection. The use of oral fluids is broadening perspectives in clinical diagnosis, disease monitoring, and decision making for patient care. Important elements determining the future possibilities and challenges in this field are also discussed.
Saliva is a clinically informative, biologic fluid (biofluid) that is useful for novel approaches to prognosis, laboratory or clinical diagnosis, and monitoring and management of patients with both oral and systemic diseases. Saliva is easily collected and stored and is ideal for early detection of disease, as it contains specific soluble biologic markers (biomarkers). Saliva contains multiple biomarkers, which make it useful for multiplexed assays that are being developed as point-of-care (POC) devices, rapid tests, or in more standardized formats for centralized clinical laboratory operations. Salivary diagnostics is a dynamic field that is being incorporated as part of disease diagnosis and clinical monitoring, and for making important clinical decisions for patient care.
Salivary diagnostics has been the subject of recent meetings and reviews, and an overview of the principles of salivary gland secretion, methods of saliva collection, and discussion of general uses can be found in a report of a meeting published in the Annals of the New York Academy of Sciences . These topics were updated in a subsequent meeting and also in a recent textbook, Salivary Diagnostics , in 2008.
Salivary diagnostics has evolved into a sophisticated science, and serves as a subset of the larger field of molecular diagnostics, now recognized as a central player in a wide variety of biomedical basic and clinical areas ( Fig. 1 ). Molecular diagnostics feeds into a wide range of disciplines including drug development and personalized medicine (pharmacogenomics), and plays a major role in discovery of biomarkers for the diagnosis of oral and systemic diseases. This is especially true because most of the biomarkers present in blood and urine can also be detected in a sample of saliva. In this article the authors focus on the use of saliva and other oral samples for the diagnosis of systemic and oral diseases.
Salivary diagnostics for systemic diseases
Historically, systemic diseases are diagnosed via (1) patient-reported symptoms, (2) examination and a medical history obtained by a physician or other medical professional, and (3) chemical analysis of blood and/or urine samples. The patient’s samples are typically sent to a remote, clinical diagnostic laboratory for determination of the levels of a broad series of markers including ions, antibodies, hormone levels, and a variety of disease-specific biomarkers. After some time (from minutes to days depending on the assay) the laboratory report is returned to the physician, and the results are then communicated to the patient. In general, oral samples are only taken if there is suspicion of an oral infection, for example a throat swab for Streptococcus pyogenes to diagnose “strep throat,” or a mucosal biopsy for suspected oral cancer. However, there has been increasing interest in the use of saliva and other oral samples for the diagnosis of oral and systemic diseases. In a sense, the rationale is obvious. If it is possible to obtain similar or identical information with an oral sample that is easy to collect and that does not require invasive procedures, the need for a blood draw would become unnecessary; this is particularly important in several populations and situations, for example, handling pediatric and geriatric patients or when access to health care is limited in remote geographic areas where phlebotomists are unavailable. A recent survey reported that dentists believe that screening for medical conditions is important, and they are willing to participate when the sample is saliva as opposed to a finger-stick.
Recently, the confirmation that an oral test for detection of antibodies to the human immunodeficiency virus (HIV) is as sensitive and specific as a blood test has led to a large increase in HIV testing at a variety of locations including emergency rooms, sexually transmitted diseases clinics, community health centers, bath houses, and most recently in dental settings. The ability to accurately detect antibodies to HIV strongly suggests the potential to detect antibodies to many other pathogens. Indeed recent literature documents this for a large number of viral and bacterial pathogens.
Oral samples that are useful for the diagnosis of systemic diseases include saliva, gingival crevicular fluid (GCF), oral swabs, dental plaque, and volatiles. Indeed, published data indicate the successful use of all of these types of oral samples to detect or predict susceptibility to systemic diseases.
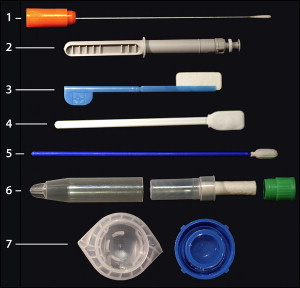
The ability to accurately assess biomarkers in samples obtained from the oral cavity depends on the biochemical nature of the marker, the source and type of sample being taken, and the mechanism by which the marker enters the oral cavity. The most widely used type of oral sampling comprises a swab that collects a DNA sample. This method has been employed for many years in forensic studies and more recently for single nucleotide polymorphism (SNP) analyses for mutations associated with specific diseases. Although a DNA sample can be collected from a wide range of sites on or in the human body, oral sampling has been used most often because of the ease of the sampling procedure, that is, a buccal brushing that is placed in a stabilizing transport medium and sent off to a laboratory for evaluation. The commercial success of genotyping individuals for disease-related DNA sequences, while still somewhat controversial for its medical value, is not questioned for its scientific accuracy. Several companies have developed kits for collection of oral swabs for this purpose. Genomic profiles are returned within weeks that can predict ancestral origins and susceptibility to several diseases. Fig. 2 presents examples of a selection of commercially available devices for collection of oral samples. Note that some of these devices (#3, #4, and #5) are shipped with a stabilizing solution for transport of oral samples to a testing laboratory. The salivette (#6) contains a cotton pad that is placed in the mouth and chewed; the pad is returned to its carrier and closed. The saliva sample is then recovered from the pad by centrifugation.
In terms of the number of publications, the second major use of oral samples is for the quantitation of steroid hormone levels. Assays are commercially available for cortisol, estriol, estrogen, and testosterone, and consistently provide accurate detection of these hormones. However, salivary levels do not correlate well with serum levels in the case of conjugated steroid hormones. Thus, whereas dehydroepiandrosterone (DHEA) can be reliably monitored in saliva and the measurements reflect blood levels of the hormone, the sulfated derivative of the steroid, DHEAS, can be measured in saliva, but the levels are not correlated with serum levels. The reason for this discrepancy appears to be the route of entry of the hormone into the oral cavity. DHEA as a steroid can readily cross the phospholipid membrane of epithelial cells lining the blood vessels, so that elevated serum levels translate as elevated saliva levels by simple diffusion of the hormone. The addition of the charged sulfate group, however, impedes membrane transport and the substance detected in saliva likely represents leakage from the blood rather than diffusion. These observations raise the general issue of a qualitative versus quantitative assay for biomarkers. When qualitative (ie, yes/no) results are needed, as in the case of pregnancy or bacterial and viral infections, saliva sampling will generally be useful. When a quantitative result is needed, for example when analyzing glucose or DHEAS levels, one must determine the saliva/plasma ratio. If this ratio is close to 1, as it is for ethyl alcohol and unconjugated steroid hormones, then quantitative salivary testing is feasible; if not, then a quantitative salivary-based assay will not be suitable for that biomarker.
The application of salivary diagnostics for systemic diseases received a major boost in 2002 as a result of a program initiated by the National Institute of Dental and Craniofacial Research (NIDCR), “Development and Validation Technologies for Saliva Based Diagnostics.” This program was designed to establish collaborative research teams between engineers with skills in nanotechnology and microfluidic techniques and scientists from the oral biology community, to develop portable POC diagnostic platforms for rapid detection and analysis of oral biomarkers. Initially 7 research teams were funded by this program, and 4 of these projects were renewed in 2006. The currently funded teams are led by Dr David Walt (Tufts University, Medford, MA) who is monitoring chronic obstructive pulmonary disease (COPD) and cystic fibrosis, Dr John McDevitt (Rice University, Houston, TX) who is developing biomarkers for acute myocardial infarction, Dr David Wong (University of California, Los Angeles, CA) who is focusing on detection of oral cancer, and Dr Daniel Malamud (New York University, New York, NY) who is developing a multiplexed test for HIV, tuberculosis, and malaria. All of these projects use advanced techniques for rapid POC diagnostics for detection of the relevant biomarkers.
A summary of selected molecules that have been accurately detected in saliva is presented in Table 1 .
| Analyte | Examples | References |
|---|---|---|
| Hormones | Melatonin, insulin, epidermal growth factor, leptin | |
| Steroids | Cortisol, androgens, (testosterone), estriol, estrogen, progesterone, aldosterone, DHEA | |
| Antibodies | IgG, IgA, sIgA, IgM | |
| Growth Factors | EGF, NGF, VEGF, IGF | |
| Cytokines and Chemokines | IL-1β, IL-8, IL-6, MCP-1, CX3CL1, GRO-1α, troponin I, TNF-α | |
| Nucleic Acids | Human DNA, microbial DNA, mRNA, siRNA, microRNA (miR-125a and miR-200a) | |
| Proteins | 100–1000 proteins | |
| Drugs | Drugs of abuse (NIDA-5), ethanol, therapeutic drugs, anticonvulsants, antipyretics/analgesics, antineoplastic agents, antibacterial agents, bronchodilators, cotinine |
Salivary Biomarkers in Cardiovascular Disease
There are numerous published reports demonstrating that C-reactive protein (CRP) can be monitored in salivary samples; however, CRP remains a nonspecific inflammatory response factor that increases in many conditions including periodontal diseases. Similarly, salivary immunoglobulin levels are known to increase in association with coronary artery disease, but once again immunoglobulins, particularly salivary IgA, are elevated in response to many local and systemic conditions. Recently, Floriano and colleagues reported that a group of salivary biomarkers can complement findings of an electrocardiogram (ECG) following an acute myocardial infarction. These markers, including CRP, myoglobin, and myeloperoxidase, in combination with an ECG, showed a highly significant correlation with myocardial infarct patients as compared with healthy controls. Salivary biomarkers have also been incorporated into POC devices for the rapid assessment of cardiovascular disease (CVD) with potential association with distinct disease stages, demonstrating promising results in identifying CVD. Elevated salivary lysozyme levels, a biomarker for oral infection and hyperglycemia, has also shown a significant association with hypertension, an early stage of CVD. Despite the progress made in biomarker discovery, robust clinical studies are required to validate salivary biomarkers for CVD and its different clinical stages.
Salivary Biomarkers for Renal Disease
Walt and colleagues and Arregger and colleagues reported on a series of salivary markers that were associated with end-stage renal disease. The list of markers included cortisol, nitrite, uric acid, sodium, chloride, pH, amylase, and lactoferrin. In a subsequent study by these same investigators, colorimetric test strips were used to monitor salivary nitrate and uric acid before and after hemodialysis. It was suggested that a salivary test could be used by patients to decide when dialysis is required, thereby eliminating unnecessary visits to a dialysis clinic. Salivary phosphate has been successfully used as a clinical biomarker for hyperphosphatemia, which is an important contributor to cardiovascular calcification in chronic renal failure (CRF). In this clinical study, 68 patients undergoing hemodialysis (HD) and 110 patients with various degrees of CRF were evaluated. Both HD and CRF patients had significantly higher salivary phosphate levels than healthy control subjects. Furthermore, evaluation of phosphate levels in saliva correlated positively with serum creatinine and the glomerular filtration rate. Thus, salivary phosphate may provide a better marker than serum phosphate for the initiation of treatment of hyperphosphatemia in CRF and HD. These results may also offer new approaches in hyperphosphatemia therapy by establishing measures to bind salivary phosphate in the oral cavity before saliva is swallowed.
Salivary Biomarkers in Psychological Research
Stress and pain are often interrelated events. Investigators have attempted to distinguish them using a variety of model systems that induce either stress or pain, and subjects are monitored for changes in salivary biomarkers. Typical markers that have been identified include salivary amylase, cortisol, substance P, lysozyme, and secretory IgA. Pain responses in dental pulp have been specifically associated with neuropeptides including calcitonin gene-related peptide (CGRP), substance P, neurokinin A, and neurokinin P. Salivary testosterone levels have been associated with increased aggressive behavior and also with athletic activities. Several reports relate cognitive behavior to levels of tryptophan and serotonin, the latter being monitored in saliva. It should be pointed out that for studies in psychological and behavior fields POC collection of saliva samples can play a key role, as a blood draw may induce both stress and pain in some individuals.
Salivary Markers for Non-oral Malignancies
The search for biomarkers for a variety of malignancies has been ongoing for decades. Once such biomarkers are detected in serum, it is a natural progression to look for these same markers in saliva. The ability to detect specific markers, particularly for malignancies that have few early symptoms such as ovarian and pancreatic cancer, would have tremendous impact on survival rates. Mutations of the tumor suppressor p53 were first reported for salivary gland adenomas in 1992 and were subsequently described in a pilot study of saliva from breast cancer subjects. Subsequently, there were reports of elevated levels of the cancer antigen CA15-3 and the oncogene c-erB2 in women with breast cancer as compared with controls. Chen and colleagues identified the tumor marker CA125 in saliva of subjects with malignant ovarian tumors. Other studies have reported down-regulation of the tumor suppressor DMBT1 in mammary tumors in mice and humans. Zhang and colleagues have identified 4 mRNA biomarkers that could distinguish pancreatic cancer subjects from pancreatitis and control subjects. It is likely that there will be an increased effort to substantiate and extend these findings in a variety of solid tumors in order to develop an early diagnostic profile.
Diabetes Biomarkers
Because of the large diabetic population, combined with the current epidemic of type 2 diabetes, an oral test to monitor blood glucose would be highly desirable. Unfortunately, while it is relatively easy to measure salivary glucose, because of the multiple sources of this material in the oral cavity salivary glucose levels do not correlate with blood glucose levels. However, several other approaches are under investigation. A recent report by Rao and colleagues demonstrated a unique proteomic signature in saliva obtained from type-2 diabetics as compared with control saliva, with 65 proteins showing greater than a 2-fold change. Many of these proteins were associated with metabolic and immune regulatory pathways. While further studies are clearly needed, these findings suggest that there may indeed be a unique salivary biomarker profile associated with diabetes. Another interesting approach to detect type 1 diabetic hyperglycemia involves measuring exhaled methyl nitrate. These investigators demonstrated a correlation between blood glucose levels and exhaled methyl nitrate, presumably because of interaction of superoxide dismutase with nitric oxide as a by-product of elevated oxidative reactions.
Finally, Strauss and colleagues have proposed using gingival crevicular blood as a measure of blood glucose. In a study of 54 subjects, blood obtained during a routine periodontal examination was collected and compared with blood obtained with a finger-stick. The study showed good correlation between samples collected from these 2 sites.
Saliva Tests for Forensics
Salivary tests have been used for a wide variety of forensic studies. Samples can be obtained from drinking glasses, cigarette butts, envelopes, and other sources, then used to detect blood-group substances or salivary genetic proteins (primarily proline-rich protein polymorphisms). Approximately 85% of individuals secrete blood-group antigens in their saliva, including A, B, H, and Lewis antigens, that have been used for identification of individuals in both criminal cases and paternity law suits. With the widespread use of DNA testing, samples of DNA taken from the buccal surface with an oral swab can be easily obtained by untrained individuals without the need for a phlebotomist. Saliva is often present at crime scenes, along with other body fluids, and because DNA is relatively stable in the dry state, these samples can be used to place an individual at the scene of a crime.
Salivary Diagnostics for Autoimmune Diseases
Major rheumatoid factor diseases include lupus erythematosis, scleroderma, and Sjögren’s syndrome. These autoimmune diseases are characterized by the production of autoantibodies that attack healthy tissue. Sjögren’s syndrome is a disease characterized by dryness of the eyes and mouth, and may occur as a primary or a secondary disease. The clinical symptoms in the primary form are more restricted and are associated with lacrimal and salivary gland dryness. In secondary Sjögren’s syndrome, patients undergo one of the aforementioned autoimmune diseases before Sjögren symptoms develop. In contrast, primary Sjögren’s syndrome (pSS) occurs by itself and is the third most common autoimmune disease, with a reported prevalence between 0.05% and 4.8%, mostly (90%) occurring in women.
For decades, the pSS diagnosis has been based on oral examination, detection of blood biomarkers (autoantibodies to self-antigens [SS-A and SS-B]), rheumatoid factor, and antinuclear antibodies, and by obtaining a confirmatory salivary gland biopsy. Patients with pSS have a 40-times higher risk of developing lymphoma, a fatal lymphocytic cancer. By contrast, patients with secondary Sjögren’s syndrome tend to have more health problems because they suffer from a primary condition as well as Sjögren’s syndrome. These patients are also less likely to have the antibodies associated with the pSS.
More recently, a panel of salivary biomarkers that can distinguish pSS patients from healthy subjects has been reported by Hu and colleagues. Using cutting-edge proteomics and genomics technologies, investigators searched globally for markers in saliva from pSS patients and healthy controls, and found that whole saliva (ie, the combination of saliva in the mouth plus saliva from the individual salivary glands) contained a series of biomarkers that could detect pSS. In addition, the proteomic and genomic profile of these salivary markers reflected the damage to glandular cells, activated antiviral immune response, or programmed cell death known to be involved in pSS pathogenesis. The value of these candidate salivary biomarkers for pSS diagnosis has been confirmed by quantitative real-time polymerase chain reaction (qRT-PCR) and immunoblotting techniques by the same investigators. Similar to pSS, the progress made in cataloging oral biomarkers derived from the salivary proteome has provided a unique opportunity and a novel approach for the future use of salivary diagnostics in many other conditions.
Salivary Biomarkers for Infectious Diseases
This topic was recently reviewed and is only be briefly summarized here. The previous review identified 23 viruses that could be identified in salivary samples by specific antibody reactivity, antigen detection, or nucleic acid via PCR. These viruses include a large range of herpes viruses, hepatitis viruses, HIV, human papillomavirus (HPV), influenza virus, and poliovirus. Fourteen bacterial pathogens were detected (by antibody, antigen, or nucleic acid), including Escherichia coli , Mycobacterium tuberculosis , Helicobacter pylori , Treponema pallidum , and a wide range of streptococcal species. Nonviral and nonbacterial infectious agents including Candida albicans , Toxoplasma gondii , and Schistosoma mansoni were detectable, typically by antibodies to these infectious agents. These pathogens are responsible for both systemic and oral diseases. Tests for these and for many other pathogens are currently under development by a large number of commercial and academic entities, so that it is likely that additional salivary-based tests for infectious diseases will continue to emerge. Some of the common pathogen- and nonpathogen-induced oral diseases and the role of saliva in their diagnosis are now described.
Salivary diagnostics of common oral diseases
The physicochemical and biochemical properties of saliva along with its complex composition endows this fluid with multiple functions, including: antibacterial, antiviral, and antifungal properties; buffering capacity for plaque acids; digestive activity (amylase, protease, nuclease enzymes) needed for food mastication; mineralizing agents for protection and repair of hard tissues; lubricant and viscoelastic properties essential for the maintenance of oral health; and protective and repairing fluid for mucosal surfaces. Saliva is a hypotonic biofluid composed of 99.5% water and 0.5% ions (eg, potassium, calcium, chloride, sodium, and phosphates), and organic micro- and macromolecules (eg, amino acids, histatins, cystatins, defensins, statherins, lysozyme, proline-rich proteins, carbonic anhydrases, peroxidases, lactoferrin, mucins, secretory immunoglobulins, and lipids, among others). The origin of these salivary components is diverse and complex, and they are not reviewed here. Whole saliva can be easily collected with stimulating agents (using paraffin for mastication, or using citric acid or sour candy drops on the tongue) or without stimulation. The unstimulated whole saliva is often used in diagnostics, as stimulated whole saliva contains a diluted concentration of biomarkers that may be difficult to detect.
Another oral fluid of interest for clinical diagnostics is the GCF, which is an interstitial biofluid or inflammatory transudate that flows out via the gingival crevice and contains: cells (desquamated epithelial cells, neutrophils, lymphocytes and monocytes, and pathogens such as bacteria); electrolytes similar to plasma (eg, potassium and calcium); and organic components also similar to plasma (eg, albumin, globulins, complement s, protease inhibitors, lactate, urea, and multiple enzymes). The GCF has a protective role in the oral cavity by removing potentially harmful cells, molecules, and pathogens, and also has an antibacterial role by virtue of its pathogen-neutralizing antibodies.
Many of the salivary or GCF-derived molecules are used as diagnostic biomarkers for oral diseases including oral cancer, and conditions caused by fungi ( Candida species), viruses (HPV, Epstein-Barr virus [EBV], cytomegalovirus [CMV]), and bacteria (multiple species involved in periodontal diseases and caries). In many instances, pathogen-induced oral diseases have been reported as opportunistic or secondary infections, and are referred to as early manifestations of the acquired immunodeficiency syndrome (AIDS) in HIV-infected subjects. The frequency of many AIDS-related oral manifestations varies, but increases in the absence of highly active antiretroviral therapy (HAART), and may indicate inadequate HAART treatment, development of drug resistance, or therapeutic failure.
Salivary Diagnostics in Oral Squamous Cell Carcinoma
Oral squamous cell carcinoma (OSCC) is the most common malignancy of the oral cavity among oral cancers (eg, adenocarcinomas, lymphomas, sarcomas, verrucous or mucoepidermoid carcinomas, malignant melanoma, and Kaposi sarcoma), accounting for more than 90% of clinical cases and ranking among the top 10 types of cancers worldwide. However, oral cancers have also been reported with less frequency in the oral mucosa, tongue, pharynx, lips, gums, palate, salivary glands, tonsils, and sinuses. Epidemiologic data have shown an increased incidence and mortality of oral cavity cancers in many countries. The latter is associated with risk factors including tobacco, alcohol, oral pathogen infections, environmental factors, and poor oral hygiene. Classically, clinical diagnosis of oral cancer has been based on visual and palpation assessment, followed by biopsy and histopathological evaluation. However, this clinical assessment has been broadened by use of magnetic resonance imaging and computed tomography ; toluidine blue staining, and light-based detection techniques. More recently, detection of biomarkers in saliva has emerged as a novel approach for the diagnosis of OSCC and its developmental stages including initial process, invasion, recurrence, and treatment. A comprehensive description of these oral cancer biomarkers has been previously described, including oncogenes (eg, C-myc, c-Fos, C-Jun), anti-oncogenes (eg, p53, p16), cytokines (eg, transforming growth factor β1, interleukin [IL]-8, IL-1β), growth factors (eg, vascular endothelial growth factor, epidermal growth factor, insulin-like growth factor), extracellular matrix-degrading proteinases (MMP1, MMP2, MMP9), hypoxia markers (HIF-α, CA-9), epithelial-mesenchymal transition markers (eg, E-cadherin, N-cadherin, β-catenin), epithelial tumor factors (CYFRA 21-1), cytokeratins (CK13, CK14, CK16), micro RNA molecules, and hypermethylation of cancer-related genes (p16 and DAP-K). These biomarkers have been defined using molecular, transcriptomic, genomic, proteomic, metabolomic, and phenotypic techniques. However, further development and validation of these biomarkers is needed for routine implementation in clinical diagnostics to assist with early cancer detection, risk assessment, and response to therapies. Refinement of a panel of soluble salivary biomarkers will depend on their stability and accuracy of detection, incorporation into sensitive and reproducible assays easy to perform, high sensitivity and specificity to indicate specific diseases and their stages of development, easy quantification in the clinical laboratory, and cost-effectiveness integration into clinical diagnostic algorithms.
Salivary Diagnostics in Oral Fungal Diseases
The oral cavity of immunocompetent individuals contains resident microbiome coexisting under a delicate immunophysiological balance and including an important fungal component known as the oral mycobiome. The latter includes culturable and nonculturable fungi, some of which may be pathogenic, causing common oral diseases such as oropharyngeal candidiasis (OPC), frequently observed in immunocompromised individuals. A recent study characterized the oral mycobiome of 20 healthy individuals showing that Candida species were the most frequently isolated fungi (present in 75% of participants), followed by Cladosporium (65%), Aureobasidium , Saccharomycetales (50% for both), Aspergillus (35%), Fusarium (30%), and Cryptococcus (20%). There are numerous factors that can disturb the balance of microorganisms in the oral microbiome and mycobiome, predisposing individuals to fungal diseases, including: physiologic changes that occur in the geriatric and pediatric populations and during pregnancy; disturbances of soft and hard tissues caused by lesions or poor oral hygiene; prolonged use of antibiotics with a broad antimicrobial spectrum; extended use of steroids that impair the immune system; nutritional deficiencies in micro- or macronutrients; endocrinological malfunction associated with diseases such as hypothyroidism; chemotherapy- and radiotherapy-induced immunosuppression due to cancer; immunodeficiencies caused by pathogens such as the HIV or congenital defects such as thymic aplasia; Xerostomia; autoimmune diseases (Sjögren syndrome); use of prosthodontic appliances; and diabetes. Mycotic infections of the oral cavity show different etiology, pathogenesis, and clinical forms. Primary OPC has been described as pseudomembranous, erythematous, and hyperplastic; while secondary OPC has been described as a chronic mucocutaneous presentation. OPC, being one of the most common oral diseases, occurs as a mixed yeast-bacterial biofilm infection and it is most commonly caused by Candida albicans . However, other Candida species are also seen in medically compromised patients with a history of liberal use of azoles. Classically the diagnosis of oral mycoses, including OPC, is based on an oral clinical examination along with the collection of oral specimens (swab, sputum, or saliva) for clinical laboratory analysis. The latter involves in vitro culture to isolate and identify the etiologic agent, direct microscopic analysis for pathogen visualization, and histopathological staining to confirm the etiologic agent and assess the severity of tissue damage. To date, saliva samples for clinical diagnosis of fungal infections are only used for pathogen isolation and not for direct clinical assay applications. The performance of a commercial enzyme-linked immunosorbent assay (ELISA) kit to detect Candida ’s mannan antigen in oral rinse solutions has been reported, but further assay optimization is needed for oral specimens. Experimental attempts have also been made to detect salivary IgA or IgG antibodies to Candida , but immunodiagnosis remains elusive because of differences observed in sensitivity and specificity of different assays when detecting various Candida antigen preparations.
Salivary Diagnostics in Oral Diseases Caused by Viruses
Oral diseases caused by viruses are prevalent, including papillomaviruses (HPV associated with oral cancer—OSSC—and oral warts) and herpesviruses (EBV causing hairy leukoplakia and also associated with various types of lymphoid and epithelial malignancies; cytomegalovirus [CMV] causing opportunistic infections after solid organ transplantation, retinitis, gastrointestinal and neurologic disorders, and oral ulcerations; herpes simplex viruses 1 and 2 [HSV-1 and HSV-2] and varicella zoster virus [VZV], also causing oral ulcerations of the aphthous type; and human herpesvirus 8 [HHV-8] causing oral and systemic Kaposi sarcoma). These oral diseases have been more frequently reported in immunocompromised patients because of impairment of the immune system, especially those with HIV/AIDS not receiving HAART, which represents more than 70% of people residing in countries where the AIDS epidemic is most devastating. On initiation of HAART, HIV/AIDS patients show lower prevalence of some of these oral diseases (hairy leukoplakia and Kaposi sarcoma), but other conditions continue or may be even more prevalent under HAART (oral warts, oral cancers, salivary gland disease, and oral lesions associated with immune reconstitution inflammatory syndrome [IRIS]). The clinical diagnosis of the oral diseases and viral agents described here is based on clinical examination supported by confirmatory clinical laboratory testing, including histopathological staining of tissue specimens, microscopic visualization of lesions and pathogens, virus isolation from clinical specimens, and nucleic- and immunoassays for detection of viral and host biomarkers. For instance, the standard approach for HIV clinical laboratory diagnosis has been testing serum or plasma samples in a sensitive ELISA followed by a Western blot if the ELISA is positive. However, oral fluids have also been successfully used in laboratory diagnostics to detect HIV antigen and antibodies in different nucleic- and immunoassay formats such as qRT-PCR, ELISA, rapid test, POC, and microfluidic diagnostic devices. In addition, HIV-neutralizing innate immune factors such as defensins have also been successfully detected in saliva using sophisticated experimental methodologies such as liquid chromatography-tandem mass spectrometry, which involves limited sample manipulation and can be easily automated.
Experimental detection of HPV in saliva samples has utilized nucleic acid assays such as HPV DNA amplification by PCR, and this methodology has also been used to detect different HPV types. Antibodies to HPV have been simultaneously tested in serum, saliva, and oral mucosal transudate specimens, yielding promising results when using oral fluids, but further optimization has also been recommended as a reliable alternative to serum HPV testing.
The EBV DNA load in blood and saliva detected by PCR has shown similar results in cohorts of HIV-infected patients. The nested PCR technique has been used to consistently detect CMV in subgingival plaque, unstimulated saliva, and peripheral blood of patients with chronic periodontitis, and it has been reported that saliva is as reliable as urine for CMV detection in large screening programs. More recently, saliva specimens have been successfully used for direct genotyping of CMV strains in a new PCR-restriction fragment length polymorphism (RFLP) method, coupled with capillary electrophoresis fragment detection for genotyping. Comparative nested PCR analyses of saliva and peripheral blood specimens have consistently demonstrated HSV-1 detection with similar frequencies in both types of samples. Similarly, reliable detection and quantification of nucleic acids for HSV-1, HSV-2, and VZV in oral fluids have been reported. There is a new standardized liquid phase–based saliva collection system, followed by a fully automated viral nucleic acid extraction and RT-PCR, using commercially available in vitro diagnostics/Conformité Européene labeled molecular assays. Lastly, shedding of HHV-8 in saliva has also been demonstrated using PCR and immunohistochemistry, and HHV-8 load in blood, serum, and saliva have shown comparable titers by qRT-PCR.
The simultaneous detection of viruses in oral fluids using different assays with multiple applications is an emerging field. Many of these assays are changing to incorporate multiplexing capabilities and to take advantage of nanotechnology approaches, yielding automated, reliable, and sensitive diagnostic devices. However, these novel detection systems require further optimization and validation prior to implementation in routine clinical diagnostics.
Salivary Diagnostics in Oral Diseases Caused by Bacteria
Caries and periodontitis are the most commonly known polymicrobial-driven diseases of the oral cavity. Periodontal disease is a chronic inflammatory process of the periodontium in response to bacterial plaque deposited on the adjacent teeth. Bacterial species form biofilms, destroy the alveolar bone and periodontal ligament, induce gingivitis, cause apical migration of the epithelial attachment resulting in the formation of periodontal pockets, and induce irreversible loss and exfoliation of the teeth. If left untreated, gingivitis may progress to periodontitis, leading to tooth loss and severe lesions of soft and hard tissues. Periodontitis is also linked to systemic illness, such as CVD and diabetes. Caries is also caused by bacterial plaque that in combination with fermentable carbohydrates produces acids (eg, lactic acid) that lower the pH at the surface of the tooth, compromising the enamel, dentin, and cementum, and ultimately affect the structural integrity of the tooth.
Clinical diagnosis of periodontal disease is based on an oral examination, consisting of inspection of the gingival tissue on the buccal and lingual side of every tooth, conducting a periodontal screening and recording pocket depths for each tooth, checking attachment level, measuring plaque index, testing bleeding on probing, testing tooth mobility, and taking radiographs to assess bone loss. Caries are also clinically diagnosed on visual examination and by taking radiographs. In both oral diseases, identification of the etiologic agents may be carried out. For this, oral specimens including plaque, GCF, and saliva are sent to and analyzed in diagnostic laboratories. Isolation of bacterial species from oral specimens using classical in vitro methods is only possible for cultivable species such as Porphyromonas gingivalis , Treponema denticola , and Tannerella forsythia present as a complex biofilm in destructive periodontitis, and Streptococcus mutans and Lactobacillus sp frequently found in caries. However, the majority of the oral bacterial species are uncultivable. For instance, the oral microbiota contains more than 700 individual taxa with approximately 200 characterized bacterial species and only about 100 of them representing cultivable strains in vitro. To bridge this gap, novel approaches in salivary diagnostics have been developed to characterize the role of the uncultivable microbiome in disease initiation and progression. Other studies are conducting a comparative analysis of salivary proteomic profiles in patients with periodontitis and healthy subjects, showing distinctive profiles with alterations of salivary proteins in the presence of periodontal inflammation, which may contribute to the improvement of periodontal diagnosis. Recently, a clinical study was conducted in which 100 individuals were enrolled either into a group of healthy/gingivitis subjects or into a group of subjects with periodontitis to identify pathogen and host-response salivary biomarkers correlated with periodontitis. For this purpose, a rapid POC chairside diagnostics was utilized, which had the capacity to characterize early stages of periodontal infection and its progression to disease. Whole saliva was collected and analyzed using antibody arrays to measure the levels of multiple proinflammatory cytokines and bone resorptive/turnover markers. Salivary biomarker data were correlated to comprehensive clinical, radiographic, and microbial plaque biofilm level (measured by quantitative PCR) to generate periodontal disease identification models. As previously described, biomarkers such as MMP-8 and -9 (matrix metalloproteinases) were elevated in subjects with advanced periodontitis, which was predicted when assessing multiple combinations of salivary biomarkers (eg, MMP-8 and -9 and osteoprotegerin) along with red-complex anaerobic periodontal pathogens (eg, Porphyromonas gingivalis or Treponema denticola ). In addition, disease severity was also predicted when obtaining elevated salivary MMP-8 and T denticola biofilm levels. This approach proved the usefulness of monitoring salivary and host-response biomarkers for an oral disease. Studies are ongoing to apply this approach to the longitudinal predictions of disease activity. A similar POC diagnostic approach was previously developed as a portable microfluidic device consisting of a chip-based immunoassay to detect biomarkers of periodontal disease in saliva.
The clinical value of salivary proteomic biomarkers in periodontal disease diagnosis is under experimental development and is based on profile changes in molecules involved in inflammation, collagen degradation, and bone loss. Despite this progress, some of the biomarkers identified are not disease specific. As with salivary proteomics, salivary transcriptomics and genomics in high-throughput platforms have also been developed using oral diseases as models, but face similar challenges as described above.
In addition to using plaque specimens for conventional bacterial isolation methods and saliva samples for proteomic biomarker profiling, GCF specimens have also been tested by ELISA to assess differential expression of specific host biomarkers (eg, RANKL and cathepsin-K indicators of osteoclast activity) for the experimental diagnosis of periodontal disease, demonstrating the use of GCF specimens in oral diagnostics. In fact, detection of GCF constituents (mostly inflammatory mediators) in saliva is the current focus of most saliva-based tests for periodontal disease.
The value of salivary diagnostics in caries has also been reported. An experimental assay was developed using biomarkers (genetically determined oligosaccharide profiles present on salivary glycoproteins) for caries risk assessment with prognostic value for caries susceptibility. Evaluation of this unique assay is under way for future diagnostic applications.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


