The purpose of this article was to describe the rootless eruption of a mandibular permanent canine in a 10-year-old boy; his mandible had been fractured in a car accident. The fracture was at the region of the developing canine, resulting in arrested root formation and causing abnormal, rootless eruption. Current theories on tooth eruption and the important role of the dental follicle in the process of eruption are discussed.
Tooth eruption is the physiologic process causing the intrabony movement and migration of a tooth from its site of formation in the bone through the alveolar process to its functional position in the oral cavity. Tooth eruption has been divided into 3 stages: preeruption, prefunctional, and functional.
The mechanisms of tooth eruption are not well understood, and numerous theories have been suggested. These include root growth and elongation, alveolar bone growth and remodeling, development of the periodontal ligament, and increased vascular (capillary) pressure in the pulp or in the periapical space.
Experimental studies have emphasized the important role of the dental follicle and proposed that it is required for tooth eruption. It was stated that tooth eruption does not take place without the dental follicle. It has been reported that surgical removal of the dental follicle compromises tooth eruption.
Eruption of a tooth with little or no root development is extremely rare. Only a few cases have been reported on rootless eruption of permanent teeth. Rootless teeth have been reported to be associated with neonatal teeth or as a result of irradiation. Abnormal rootless eruption of teeth was reported in a patient with congenital renal disease, and a rootless mandibular second premolar was reported under a deciduous molar with no signs of decay or infection.
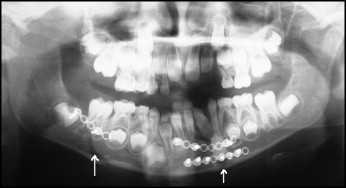
This report describes a rare case of rootless eruption of a mandibular permanent canine after mandibular double fractures in a boy who, at age 7, was injured in a car accident. The fracture lines were along the developing left permanent canine and below the right first permanent molar. He was surgically treated with rigid fixation ( Fig 1 ). The left permanent canine had complete crown formation with the beginning of root development. The fixation was eventually removed, and he was seen annually by his oral surgeon, who took panoramic radiographs. The radiograph taken 1 year postsurgery, at the age of 8 years, showed bone healing in the fractured zones. The mandibular left permanent canine appeared somewhat rotated, and the mandibular left permanent lateral incisor had an obliterated root ( Fig 2 ).
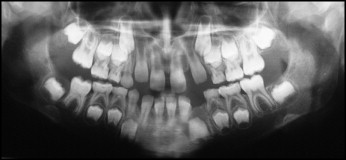
At the age of 9 years, the boy’s rotated canine continued its eruption path with no signs of root development. At that time, the mandibular right permanent second molar became obliquely impacted for unknown reasons ( Fig 3 ).

Clinical examination and treatment
The patient was first referred and examined for orthodontic consultation and treatment at the age of 10 years ( Figs 4 and 5 ). He had a Class I malocclusion in the late mixed dentition with spaces between the maxillary incisors. The mandibular left permanent canine had not erupted, whereas the right canine was fully erupted. Scar tissue of the previous surgical fracture repair was evident in the gingiva below the mandibular incisors.
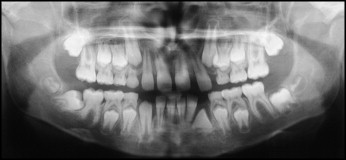

The panoramic radiograph shows the teeth in the late mixed dentition, including the developing buds of the mandibular third molars. The mandibular left permanent canine appears completely rootless and rotated and is unerupted. The mandibular left permanent lateral incisor has an obliterated root, and the right second permanent molar appears horizontally impacted.
Treatment objectives for this patient included maintaining the Class I interarch relationship, closing the maxillary anterior spaces to provide space for the eruption of the left permanent canine, surgically exposing and orthodontically uprighting the impacted mandibular right permanent second molar, and surgically removing the rootless canine after closure of the space by moving the posterior teeth forward. Other treatment options and alternatives were also discussed with the parents regarding the poor prognosis of the rootless mandibular canine, and the unfavorable position of the impacted mandibular right second permanent molar. The parents reported that their son did not maintain good hygiene and was impatient; therefore, they sought the shortest possible treatment. It was agreed to wait and see what happened to the rootless canine, and proceed with the shorter treatment option of surgically uprighting the impacted second molar.
After the patient improved his oral hygiene, the maxillary anterior spaces were closed with a 2 × 4 edgewise appliance. This also opened the space for eruption of the maxillary left permanent canine. Interestingly, the mandibular left canine erupted with no root, as seen in the follow-up panoramic radiograph ( Fig 6 ).



