Introduction
Root resorption is an undesirable consequence of orthodontic tooth movement. The severity is unpredictable, and, despite extensive research, the etiology remains unknown. Torque has been acknowledged as a risk factor for root resorption. The aims of the study were to evaluate and quantify the extent of root resorption after the application of 2.5° and 15° of buccal root torque for 4 weeks.
Methods
Fifteen patients requiring bilateral extraction of their maxillary first premolars for orthodontic treatment were recruited to the study. By using a standardized experimental protocol, the right and left premolars were randomly subjected to either 2.5° or 15° of buccal root torque. At the end of the 4-week experimental period, the premolars were extracted. A volumetric analysis of root resorption was performed by using microcomputed tomography and measured with specially designed software.
Results
Overall, the amounts of root resorption were comparable after the application of 2.5° or 15° of buccal root torque ( P = 0.59). There was a significant difference between the 2 force levels only at the apical region ( P = 0.034). More root resorption occurred in areas of compression than in areas of tension. The variables of age and sex were not statistically significant.
Conclusions
Root resorption was evident after 4 weeks of buccal root torque application. More root resorption was seen at the apical region than at the middle and cervical regions. Higher magnitudes of torque might cause more root resorption, particularly in the apical region. As shown in previous studies, the etiology of root resorption is multi-factorial and cannot be explained by mechanical factors alone.
Root resorption is a process involving the destruction and removal of mineralized and a thin layer of unmineralized cementum and dentin. It might be physiologic or pathologic. Orthodontically induced inflammatory root resorption is a form of pathologic root resorption related to the removal of hyalinized areas of the periodontal ligament after orthodontic force application.
Orthodontically induced inflammatory root resorption is an undesirable but unavoidable iatrogenic consequence of orthodontic treatment. The severity of orthodontically induced inflammatory root resorption is unpredictable. In mild cases, the resorption might be clinically undetectable or just minor root blunting. When the resorption craters accumulate at the apex, it can be lost and the tooth permanently shortened. Linge and Linge found that 16.5% of orthodontically treated patients had root shortening of more than 2.5 mm in at least 1 tooth. Davidovitch observed that 3% to 5% of the treated population experienced excessive root resorption.
Fortunately, the long-term prognosis of most affected teeth is good. The signs of active resorption discontinue with the cessation of orthodontic force, and the longevity and functional capacity of the tooth are generally not affected. In some cases, however, the resultant reduced crown-to-root ratio can be significant and preclude certain dental treatment options, particularly in the event of future periodontal disease or trauma.
The etiology of root resorption is multi-factorial, and susceptibility can be affected by patient-related biologic risk factors such as genetic predisposition, the patient’s age, or treatment-related mechanical risk factors. Treatment-related factors are of particular interest to clinicians because these might be amenable to change via modifications to treatment mechanics. The effect of force magnitude on root resorption has been widely investigated, with most studies showing evidence of greater root resorption with higher levels of force.
Torque refers to third-order or, more specifically, torsional bends placed along the long axis of a rectangular archwire. Torque induces faciolingual or buccolingual rotation of the tooth and is measured by the relative crown and root inclinations perpendicular to the line of occlusion. Correct anterior and posterior torque values are considered essential to providing optimal esthetics, stability, and proper occlusal relationships in orthodontic treatment.
Previous investigators found torque to be a risk factor for root resorption. Kaley and Phillips observed that severe root resorption was 4.5 times more likely if subjected to torquing forces and 20 times more likely if torqued against the lingual cortical plate. Casa et al investigated the effects of lingual root torque on premolars with scanning electron microscopy. Root resorption was observed in the apical and bucco-cervical regions and increased in severity with increased magnitude and duration of forces. Similar results were seen in a second study by Casa et al using tartrate resistant acid phosphatase histochemistry and transmission electron microscopy.
Root resorption is a 3-dimensional phenomenon. Two-dimensional methods of assessment such as conventional radiographs have been shown to underestimate root resorption. Microcomputed tomography (micro-CT) is the current gold standard for the quantification of root resorption but has yet to be used to quantify root resorption after the application of controlled buccal root torque.
The aim of the study was to evaluate the extent and distribution of root resorption craters after the application of 2.5° and 15° of buccal root torque for 4 weeks. This study is a continuation of a series of studies investigating the process of root resorption developed at the University of Sydney in Australia.
Material and methods
Thirty maxillary first premolars were collected from 15 patients who required extractions for orthodontic purposes. Written informed consent was obtained from the patients and their parents or guardians before the study. Ethics approvals were obtained from the University of Ondokuz Mayis and the University of Sydney (project 10-2008/11235 of the Human Ethics Review Committee of the Sydney South West Area Health Service).
The patients, 8 girls and 7 boys (mean age, 14.3 years; range, 12.75-16.83 years), were selected according to the strict criteria described previously. All subjects completed written informed consents and questionnaires about dental history and birthplace. The right or left premolars were randomly chosen for the application of 2.5° or 15° of buccal root torque.
Each patient had an alginate impression taken of the maxillary arch. The impressions were poured in plaster for posterior appliance construction.
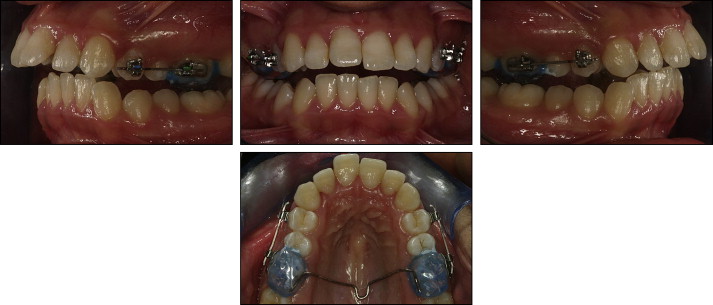
A standardized, passive transpalatal arch with acrylic occlusal coverage and a SPEED bracket (Strite Industries, Cambridge, Ontario, Canada) on the buccal aspect was constructed and bonded to the maxillary first molars with Multi Cure Glass Ionomer cement (3M Unitek, Monrovia, Calif). This provided anchorage and ensured that the desired degree of buccal root torque was fully expressed on the experimental teeth. In addition, the transpalatal arch disengaged the occlusion and ensured that the movement of the subject teeth was not impeded by occlusal interferences. Hence, the force system designed for this study had no impact on the future orthodontic treatment of these subjects.
A SPEED bracket (0.022 × 0.028 in) for the maxillary first premolar was attached to a length of beta-titanium-molybdenum alloy wire (0.021 × 0.025 in). The wire with the attached bracket was engaged in the bracket of the maxillary first molar, and the bracket for the maxillary first premolar was then bonded passively to the subject tooth with Transbond (3M Unitek). When the adjacent teeth were malaligned, the wire was bent to prevent interferences. The wire was marked 2 mm mesially and 2 mm distally to the bracket of the maxillary first premolar. The wire was then removed, and, at a point considerably mesial to the marking made 2 mm mesially to the maxillary first premolar, a 90° bend was placed by using Tweed pliers. The wire was then held with the pliers at the marking 2 mm distally to the first premolar, and either 2.5° or 15° of buccal root torque was placed in the anterior section of the wire. The amount of torque was accurately measured by holding the wire with the pliers and reading the angle of the perpendicular portion of the wire against a protractor mounted vertically on a bench.
The anterior section of the wire was cut at the marking made 2 mm mesially to the first premolar. The wire was then placed into the bracket of the maxillary first molar and engaged in the bracket of the maxillary first premolar ( Fig 1 ).
One side of each subject’s mouth was randomly designated as the heavy-torque side and the other as the light-torque side. On the light-torque side, 2.5° of buccal root torque was introduced to the wire. On the heavy-torque side, 15° of buccal root torque was introduced. The duration of the experiment was 4 weeks. Formulae derived from engineering principles were used to estimate the forces applied at the level of the bracket. The resultant forces from the application of 2.5° and 15° of buccal root torque were calculated to be 47.5 and 285 gmm (gram-millimeter), respectively.
At the end of the 4-week experimental period, the teeth were extracted by 1 of 2 oral surgeons who followed a previously established protocol to prevent damage to the root cementum. After extraction, the teeth were placed in individually marked containers of deionized water (Milli Q, Millipore, Bedford, Mass), which has previously been found to be an appropriate storage medium. The teeth were kept in the Milli Q for a minimum of 1 week, and then they were placed in an ultrasonic bath for 10 minutes to remove all residual periodontal-ligament and soft-tissue fragments. The teeth were then wiped with damp gauze and disinfected in 70% alcohol for 30 minutes before storage in Milli Q again. Before analysis, the teeth were coded and bench dried for a minimum of 48 hours. Subsequent blinded analysis of the teeth was performed by using micro-CT (N.B.).
The SkyScan 1172 (Aartselaar, Belgium) was used in the study; it enabled the nondestructive evaluation of the root resorption craters. The SkyScan 1172 is a compact, desktop x-ray system based on a cone-beam x-ray source, with a charge-coupled device camera. The teeth were scanned individually. All scans were acquired at 8-μm resolution and reconstructed by using the same parameters as in the study of Harris et al.
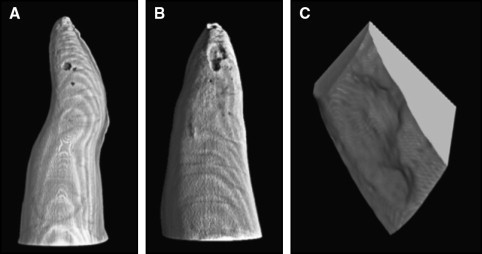
The images were obtained by using the software program NRecon (version 1.4.2) and reconstructed with VGStudioMax (version 1.2; both, Volume Graphics, Heidelberg, Germany) as previously described ( Fig 2 ). The 4 surfaces of the root (buccal, lingual, mesial, and distal) were analyzed for root resorption, and the teeth were divided into thirds (cervical, middle, and apical) to analyze the distribution of the craters. The 3-dimensional images of the teeth were saved as permanent files. The method by which the craters were acquired was recorded with respect to the x-, y-, and z-axes. Therefore, repetitions of the tests were not necessary.
The volumetric measurements of the craters were calculated by using customized convex hull software developed at the Electron Microscope Unit of the University of Sydney. All craters were measured individually and then summed to obtain the total volume of root resorption craters per tooth.
Statistical analysis
Univariate analysis of variance (ANOVA) was performed by using the Statistical Package for the Social Sciences (SPSS for Windows, version 16, SPSS, Chicago, Ill). During the statistical analysis, the raw data were transformed to better satisfy the assumptions needed for the various statistical procedures (particularly, normality of the residuals). The cube root of the volumetric readings was used to create a model for statistical analysis. Essentially, this replaces each volume by the radius of an equivalent hemispheric crater. This approach was used in previous studies. The factors used in the model were subject (random), and force and surface (fixed). Paired t tests were used to compare the amount of root resorption at specific surfaces selected by using theoretical considerations.
Results
Overall, the differences in root resorption after the application of either 2.5° or 15° of buccal root torque were not statistically significant ( P = 0.59) ( Table I shows the significance of the factors and interactions). The estimated marginal means of the cubed root volume were similar: 0.36 mm for 2.5° and 0.38 mm for 15° of torque ( Table II ) ( Figure 3 ). There was a large variation in the amount of root resorption observed with the lower torque magnitude. The amount of root resorption after 15° had a smaller distribution in general, but there were 3 outliers that experienced low amounts of root resorption with the higher degree of torque.
| Source | Dependent variable | Df | F | Significance |
|---|---|---|---|---|
| Force | Total root resorption | 1 | 0.301 | 0.592 |
| Sex | 1 | 3.204 | 0.097 | |
| Age | 1 | 4.643 | 0.051 | |
| Force | Cervical third | 1 | 0.035 | 0.370 |
| Force | Middle third | 1 | 0.041 | 0.842 |
| Force | Apical third | 1 | 5.553 | 0.034 |
| Force | Mean | SE |
|---|---|---|
| 2.5 | 0.355 | 0.035 |
| 15 | 0.382 | 0.035 |
When the results were separated and analyzed by thirds, more root resorption was noted in the apical region than at the other levels of the root (Fig 3) . A significant difference between the 2 magnitudes of torque was seen at the apical region ( P = 0.034). The differences at the middle and cervical levels were not significant ( P = 0.842 and P = 0.370, respectively) ( Table III ).


