The use of “anteriorly or posteriorly” tilted implants in a graftless approach for immediate loading the edentulous maxillae has been well documented in the literature. This treatment concept allows for rehabilitation of the edentulous maxillae with a fixed prosthesis. The purpose of this article is to describe criteria for the use of the zygomatic implant, including the expanded use of the zygoma implant in cases where failure of one of the anterior or posterior tilted implants has occurred in the All-on-Four treatment concept. Zygomatic implant placement becomes a “rescue procedure”, which allows for continuity of care without resorting to a removable denture.
The use of tilted implants in a graftless approach for immediate loading has been well documented in the literature. This treatment for fully edentulous and often times highly resorbed maxillae allows for rehabilitation with a fixed prosthesis. The purpose of this article is to describe criteria for use of the zygomatic implant, including the expanded use of the zygoma implant in cases where failure of one of the anteriorly or posteriorly tilted implants has occurred in All-on-Four treatment. Zygomatic implant placement becomes a rescue procedure, which allows for continuity of care without resorting to a removable denture.
The treatment of the edentulous maxilla using dental implants has been evolving in the last decade. The edentulous maxilla presents with unique anatomic considerations. The presence of the maxillary sinus limits the volume of the available bone for placement of implants. Because of this, implants are restricted to the premaxilla unless grafting is preformed, which commonly results in a tissue-borne overdenture appliance.
Because of a desire to maintain bone through “internal loading”, bone-grafting procedures for implant placement have been advocated to biomechanically stimulate the entire maxilla via anteroposterior distribution of implants. But to avoid grafting procedures and transitional dentures, the concept of tilting implants was developed to achieve immediate function. This idea of implant tilting moves the prosthetic support posteriorly ( Fig. 1 ). Concern about increased “bending moments” (unfavorable lateral forces) from tilted implants has not been demonstrated because posterior cantilevers are less than for axial placement and immediate cross-arch stabilization is used.
In cases where only premaxillary alveolar bone remains, the placement of zygomatic implants, used in a staged fashion, well establishes posterior support. But now, recent studies have shown favorable outcomes using zygomatic implants and immediate loading with fixed provisional prostheses.
In review of the literature, the longest-term study followed a 2-stage protocol. In 2004 Branemark and colleagues reported a cumulative survival rate (CSR) of 94.2% on a 5- to 10-year follow-up of 28 subjects using 52 zygoma implants. In a recent prospective study by Bedrossian, a CSR of 97.2% was observed following 36 subjects having received 74 zygoma implants over a 7-year period.
Patient selection
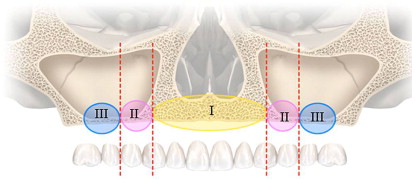
A systematic preoperative evaluation of patients is required before surgical treatment. Both surgical and prosthetic needs must be considered for a predictable outcome. The preoperative evaluation takes into consideration available alveolar bone in the different zones of the maxilla ( Fig. 2 ) and the presence or lack of a composite defect. This evaluation then determines whether the final prosthesis is a ceramo-metal bridge or profile prosthesis. Treatment is prescribed based on the availability of bone in maxillary zones. Zone I is the premaxilla, zone II is the bicuspid zone, and zone III is the posterior maxilla. An anterior tilted implant concept is considered in patients with bone in both zone I and II. The zygomatic implant concept is considered in patients who demonstrate bone in zone I only ( Table 1 ).