A woman, aged 47 years 6 months, with an anterior open bite and a left-shifted mandible was treated with a mandibular right first molar extraction and without orthognathic surgery. However, her mandibular second molar did not move mesially during treatment because of the dense lamina dura; therefore, corticision was applied only on the mesial aspect of the mandibular second molar, and a miniscrew was inserted simultaneously. Corticision was introduced as a supplemental dentoalveolar surgery in orthodontic therapy to achieve accelerated tooth movement with minimal surgical intervention. In this technique, a reinforced scalpel was used as a thin chisel to separate the interproximal cortices transmucosally without a flap. This technique was applied not to accelerate tooth movement, but to protract the mandibular molars. One miniscrew was inserted on the mesiobuccal side of the mandibular right molar for protraction and intrusion. In addition, 2 miniscrews were inserted in the buccal sides of the maxillary first and second molars and the palatal side of the maxillary first molar to intrude them for correction of the mandibular shift and the cant of the occlusal plane. Excellent occlusion and correction of the anterior open bite were achieved without surgery. At the 2-year follow-up examination, the patient had a good occlusion and showed good stability with no opening of the extraction space. A partial corticision is an effective option for facilitating movement of mandibular molars.
If the third molar is present, extraction of the mandibular first molar is a possible alternative to correct an anterior crossbite and a severe Class III molar relationship. The mandibular molars are difficult to move mesially compared with the maxillary molars because the mandible comprises thick cortical bone connected by coarse trabecular bone. The molar roots are extremely wide buccolingually, so sometimes the edentulous space cannot close.
Roberts et al used a rigid endosseous implant in the retromolar area for mesial movement of the mandibular molars. Recently, miniscrews, which are more convenient and simple and can be placed anywhere, have become popular for absolute anchorage. Several case reports have illustrated protraction of the mandibular second and third molars with miniscrews.
On the other hand, there are many approaches to shorten the time for orthodontic tooth movement, such as alveolar corticotomies, which produce a regional acceleratory phenomenon. This phenomenon is characterized by a burst of localized remodeling that accelerates healing, particularly after the surgical wounding of cortical bone. Kim et al reported a new procedure called “corticision” to accelerate tooth movement. This technique produces a minimal surgical injury to the gingiva, cortical bone, and trabecular bone around the target teeth, thereby initiating the regional acceleratory phenomenon.
This case report describes an orthodontic treatment with a partial corticision to protract the mandibular molars with a miniscrew for anchorage. With this technique, a reinforced scalpel was used as a thin chisel to separate the interproximal cortices transmucosally without a flap. Corticision was applied to only 1 aspect, not to accelerate tooth movement but to protract the mandibular molars.
Diagnosis and etiology
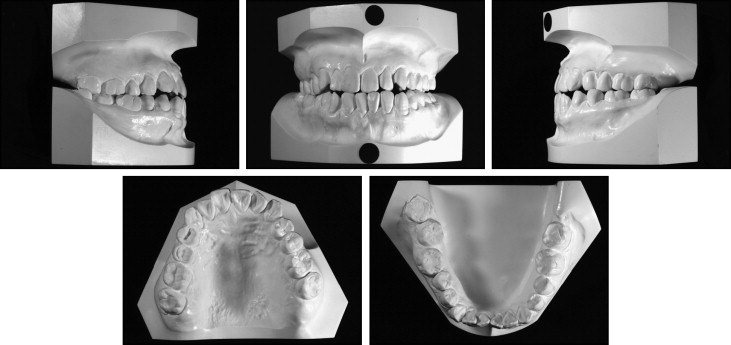
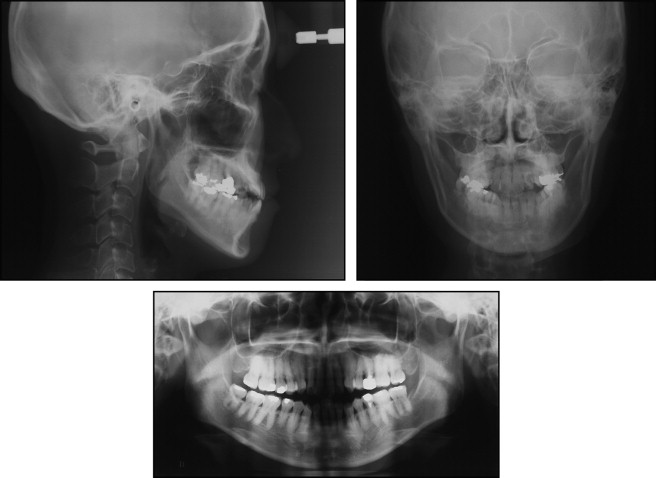
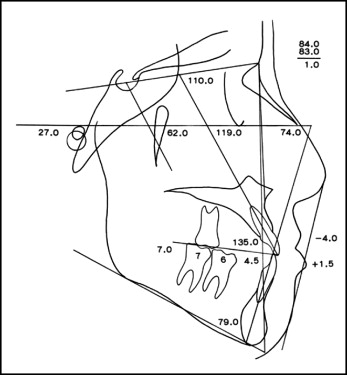
The patient was a 47-year-old woman who complained of a maxillary anterior crossbite and a mandibular lateral shift. Her father also had an anterior crossbite. Her face was asymmetric, and her chin and mandible were shifted to the left. Her lips were inclined, and the left corner was positioned higher than the right. On the smiling photo, her occlusal plane was canted ( Fig 1 ). Her maxillary dental midline was almost aligned with the facial midline, but the mandibular midline was positioned 6 mm to the left because of the mandibular shift. The left side was in crossbite except for the second molars. Her anterior teeth were in an end-to-end relationship (0 mm of overbite), and she had a mild anterior open bite. She had a mandibular right third molar that occluded with the maxillary second molar. Her molar relationships were Class I on the left side and Class III (6 mm) on the right side. Overbite was 0 mm ( Fig 2 ). Her lateral facial view showed a prominent chin and excessive lower anterior facial height ( Fig 1 ). Cephalometric analysis showed a skeletal Class III relationship (ANB, 1.0°) with a mesially positioned maxilla (SNA, 84.0°) and a forward-positioned mandible (SNB, 83.0°). The maxillary incisors were inclined labially (U1-FH, 119°), and the mandibular incisors were inclined slightly lingually (FMIA,74.0; L1-APo, 4.5 mm) ( Figs 3 and 4 , Table ). The soft-tissue analysis showed a slight protrusion of the lower lip (lower lip to E-line, 1.5 mm).

| Measurement | Japanese standard | Pretreatment | Posttreatment | Two years postretention |
|---|---|---|---|---|
| SNA angle (°) | 82.3 | 84 | 84 | 84 |
| SNB angle (°) | 78.9 | 83 | 84 | 84 |
| ANB angle (°) | 3.4 | 1 | 0 | 0 |
| MP-FH (°) | 28.8 | 27 | 24.5 | 25.5 |
| Y-axis (°) | 65.4 | 62 | 61 | 61 |
| FMIA (°) | 54.9 | 74 | 74 | 74 |
| L1-MP (°) | 96.3 | 79 | 81.5 | 80.5 |
| L1-APo (mm) | 3 | 4.5 | 3 | 2.5 |
| U1-FH (°) | 111.1 | 119 | 122 | 120 |
| U1-SN (°) | 104.5 | 110 | 113 | 112 |
| Interincisal angle (°) | 124.1 | 135 | 132 | 134 |
The panoramic radiograph showed that the roots of the mandibular right first molar were widely diverted and thick, with a dense lamina dura around the roots. The mandibular right third molar had divergent and narrow mesial and distal roots ( Fig 3 , C ).
A functional assessment showed no remarkable discrepancy between centric occlusion and centric relationship, and no temporomandibular joint problems. The mandible was shifted skeletally.
Treatment objectives and plan
I planned to maintain the anteroposterior position of the maxillary incisors since there was no significant facial profile problem, except for the slight protrusion of the lower lip. The main treatment objectives consisted of retracting the mandibular incisors to correct the incisor relationship and obtain a normal overbite. Midline correction consisted of reciprocal protraction of the mandibular right second and third molars and mandibular incisor retraction after extraction of the mandibular right first molar. After closure of the edentulous space, I tried to improve the canted occlusal plane with intrusion of the maxillary and mandibular right molars using miniscrews.
Treatment objectives and plan
I planned to maintain the anteroposterior position of the maxillary incisors since there was no significant facial profile problem, except for the slight protrusion of the lower lip. The main treatment objectives consisted of retracting the mandibular incisors to correct the incisor relationship and obtain a normal overbite. Midline correction consisted of reciprocal protraction of the mandibular right second and third molars and mandibular incisor retraction after extraction of the mandibular right first molar. After closure of the edentulous space, I tried to improve the canted occlusal plane with intrusion of the maxillary and mandibular right molars using miniscrews.
Treatment alternatives
The first treatment of choice was to correct the skeletal discrepancies, the mandibular lateral shift, and the canted occlusal plane with a combination of orthognathic surgery and orthodontic treatment. The patient, however, was fearful of surgery and the associated risks, and rejected it. The next alternative proposal was to use temporary anchorage devices for distal movement of the mandibular right molars after extraction of the third molar to correct the anterior crossbite and the shift of the mandibular dental midline to correct the mandibular asymmetry. However, the roots of the mandibular right first molar were widely divergent and surrounded by a dense lamina dura. If possible, it was desirable to intrude the right molars to correct the mandibular shift and the canted occlusal plane during the treatment. However, the retromolar miniscrew could not be implanted deep enough to intrude the mandibular molars with distalization.
The next treatment option was an unusual extraction of only the mandibular right first premolar and reciprocal retraction of the mandibular incisors and protraction of mandibular right molars to establish a Class III molar relationship. However, with a Class III molar relationship it is difficult to establish a stable occlusion. Therefore, the mandibular right first molar was extracted, the second and third molars were protracted, and the mandibular incisors were retracted reciprocally to establish the Class I relationship between the maxillary right first molar and the mandibular right second molar.
Treatment progress
First, a transpalatal arch was placed for torque control of the molars and to prevent extrusion of the molars. Then the mandibular right first molar was extracted. All maxillary teeth and the mandibular right segment were banded, bonded, and leveled, and the mandibular right second premolar and second molars were moved reciprocally. Then all mandibular teeth were bonded. After 8 months of leveling, Class III elastics were worn to correct the midline deviation and the anterior crossbite. On the panoramic radiograph at this time, the radiopaque socket of the extracted mandibular first molar was observed clearly.
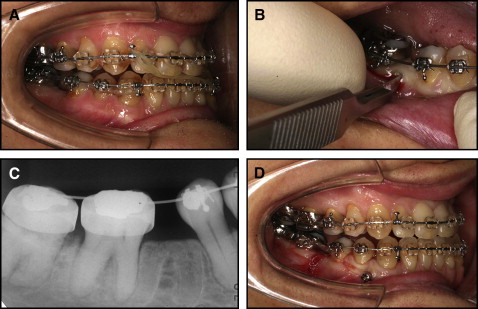
After 16 months, the anterior open bite was corrected, and the right canine relationship was Class I; however, the mandibular second molar did not move forward, and the mandibular right edentulous space remained at 8 mm. Therefore, I decided to apply corticision to the mesial aspect of the mandibular second molar to protract the mandibular second and third molars more efficiently. At this time, a 0.016 × 0.022-in beta-titanium wire was used as a working wire ( Fig 5 , A ).