Introduction
The literature on preeruptive intracoronal resorption is sparse, comprising mainly reports of single patients. This study includes 13 patients with preeruptive intracoronal resorption, forwarded for consultation regarding diagnostics and etiology. The purposes were to determine which teeth are affected by the condition and describe how the defect is manifested radiographically.
Methods
We used visual analyses of dental or panoramic radiographs.
Results
The mandibular second molar appears to be the tooth that is most often affected by preeruptive intracoronal resorption. The resorption of the dentin in the molar crown was in the initial phases often seen in the medial aspects. The dentin in the crown could also be completely resorbed. The enamel contour encircling the dentin persisted as shown on the radiographs. In 1 maxillary canine, the dentin and enamel structures were completely disorganized by the resorption processes.
Conclusions
Specialists in orthodontics are often the first to see radiographs of unerupted permanent teeth; therefore, they have a responsibility to be aware of the condition and refer these patients to an endodontist for treatment planning and prognosis before a decision is made regarding orthodontic treatment.
External and internal resorption of erupted permanent teeth is well documented in the scientific dental literature. Recently, the focus has been on the association between resorption patterns in the deciduous dentition and unexpected external root resorption in the permanent dentition.
External root resorption in permanent teeth can appear and progress without any apparent cause. Successful treatment of these patients has not been reported. External resorption can also be provoked by cysts, trauma, or pressure from erupting teeth or orthodontic appliances. In these cases, the ongoing resorption process does not normally continue when the physical pressure subsides. The resorptive defects can be repaired by a thin layer of secondary cementum.
Internal resorption is relatively rare and normally associated with physical trauma or caries-related pulpitis. The treatment involves endodontic therapy; in severe cases, extraction is needed.
Resorption of unerupted teeth is often a result of regional pathologic processes or ectopic eruption from neighboring teeth. Certain types of resorption of permanent unerupted tooth crowns have been described in case reports and also demonstrated in a textbook. Of the cited references, only Skaff and Dilzell described 2 patients; all other references reported only single patients.
Histologic studies of unerupted teeth with intracoronal resorption have shown that the change in the dentin is caused not by caries but by resorption from invagination of odontoclasts through minor defects in the enamel.
The purposes of our study were to analyze 13 patients with preeruptive intracoronal resorption, determine which teeth are affected by the condition, and describe how the defect is manifested radiographically.
Material and methods
The study included radiographs from 13 patients with preeruptive intracoronal resorption, forwarded from municipal dental services to the Department of Orthodontics, University of Copenhagen in Denmark, for consultation regarding diagnostics and etiology. The teeth affected by intracoronal resorption were 2 permanent teeth in the maxilla and 11 permanent teeth in the mandible.
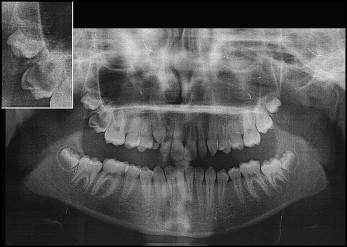
In 1 patient, normal crown morphology of a maxillary canine was seen on the radiograph before eruption, but the dentin and enamel structures were completely disorganized by the resorption processes after eruption ( Fig 1 ).

In another patient, complete resorption of the dentin was seen in the crown of a maxillary second molar, and a thin layer of enamel persisted ( Fig 2 ).
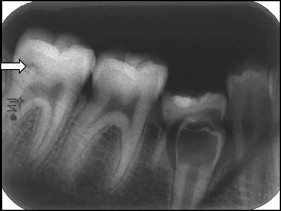
A characteristic for these preeruptive dentin defects in mandibular premolars (2 patients) is that the enamel structure appears thin on the radiographs, whereas the dentin in the crown was completely resorped. In 1 patient, a possible dentin defect was observed in a second molar ( Fig 3 ).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


