Introduction
The aim of this study was to compare the posterior tooth angulations in patients with open-bite malocclusion and normal occlusion.
Methods
Lateral cephalometric headfilms of 45 untreated open-bite subjects were compared with the lateral headfilms of 45 subjects with normal occlusion in the permanent dentition. The groups were matched for age and sex distribution and compared with t tests.
Results
The maxillary and mandibular premolars were more mesially angulated in relation to the bisected occlusal plane, and the first and second molars were significantly more distally angulated in the open-bite group in relation to the palatal and mandibular planes.
Conclusions
The maxillary and mandibular premolars were more mesially angulated in relation to the bisected occlusal plane and therefore do not compensate for the divergence of the palatal and mandibular planes as the molars do.
Highlights
- •
We compared the posterior tooth angulations in open-bite and normal occlusions.
- •
Premolars had a greater mesial angulation in the open-bite group.
- •
Molars had a greater distal angulation in the open-bite group.
Malocclusion is caused by an imbalance in the complex interactions among the facial growth pattern, causative local factors, and the lack of a dentoalveolar compensation mechanism. In particular, anterior open-bite malocclusions associated with a strong vertical component are the most challenging to treat. Combinations in vertical dysplasia are various, so that a patient with a long face can have a deepbite, and a patient with a short face is not excluded from developing an anterior open bite.
The pioneer implant studies of Björk and Björk and Skieller showed the influence of the rotation of the apical bases on the final tooth positions. Solow described in more detail the dentoalveolar compensatory mechanism, and Kim stated that in skeletal open-bite subjects the posterior teeth have a marked mesial angulation when measured in relation to the bisected occlusal plane (BOP), and a major treatment objective is to upright these teeth to facilitate bite closure. Since these reports, there have been few specific studies evaluating this dental feature, which is regarded as an anterior open-bite characteristic. Much attention has been given to the compensatory vertical dentoalveolar development of the posterior and anterior teeth in open-bite malocclusions and not to the posterior tooth mesiodistal angulations.
Therefore, the aim of this study was to test the null hypothesis that there is no difference in posterior tooth angulations in patients with open-bite malocclusion and normal occlusion.
Material and methods
This study was approved by the ethics in research committee of Bauru Dental School, University of São Paulo, Brazil, with research protocol number 20303213.2.0000.5417.
The sample size calculation, considering an 80% test power at a significance level of 5%, with a minimum mean difference to be detected of 3° and a mean standard deviation of 5°, showed that 45 subjects in each of the 2 groups were the minimum for providing reliable results. The minimum mean difference to be detected and the standard deviation of the maxillary first premolar in relation to the bisected occlusal plane were based on a previous study.
The sample, consisting of lateral headfilms of 90 (43 male, 47 female) untreated subjects in the permanent dentition, selected from the files of the Department of Orthodontics at Bauru Dental School, University of São Paulo, Brazil, was divided into 2 groups, based on the amount of overbite, regardless of cephalometric characteristics. All subjects had all permanent teeth up to the second molars.
Group 1 (open bite) consisted of lateral headfilms obtained from 45 (20 male, 25 female) untreated subjects of Mediterranean ancestry, with a mean age of 13.95 years (range, 12-19.75 years); their open bites ranged from 0.5 to 8.7 mm, with a mean of 2.68 mm. Twenty-four had Class II, 17 had Class I, and 4 had Class III malocclusions.
Group 2 (normal occlusion) consisted of lateral headfilms obtained from 45 (23 male, 22 female) subjects with a mean age of 13.83 years (range, 12-15.33 years), with overbites from 0.5 to 4.7 mm, with a mean of 3.04 mm and pleasant facial profiles, of Mediterranean ancestry.
The cephalometric tracings and landmark identifications were performed on acetate paper by 1 investigator (V.L.) and then digitized with a digitizer (DT-11; Houston Instruments, Austin, Tex).
Overbite measurement was defined as the distance between the maxillary and mandibular incisor borders perpendicular to the functional occlusal plane ( Fig 1 ).
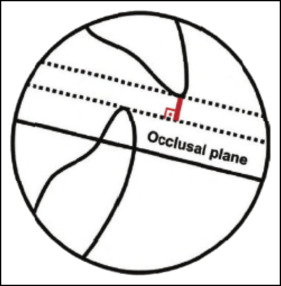
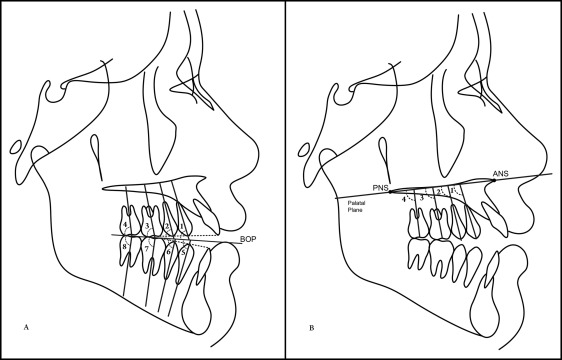
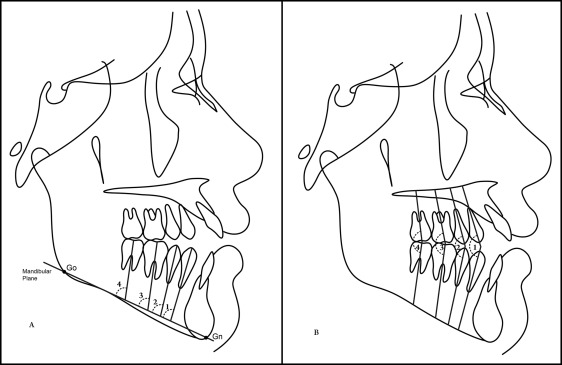
In total, 129 landmarks were identified, and 30 measurements were performed ( Table I ). Posterior tooth angulations were measured in the maxillary and mandibular arches and consisted of measuring the angles between the premolars’ (apex-cusp tip) and the molars’ long axes (furcation-center of the crown) to the BOP ( Fig 2 , A ) and to the palatal plane (ANS-PNS) ( Fig 2 , B ) and the mandibular plane ( Fig 3 , A ). The interpremolar and intermolar angulations were measured as well ( Fig 3 , B ). The BOP was obtained by bisection of the maxillary occlusal plane (from the distal buccal cusp of the maxillary second molar to the incisal edge of the most extruded maxillary central incisor) and the mandibular occlusal plane (from the distal buccal cusp of the mandibular second molar to the incisal edge of the most extruded mandibular central incisor).
| Maxillomandibular relationship (°) | |
| SNA | SN to NA angle |
| SNB | SN to NB angle |
| ANB | NA to NB angle |
| Growth pattern | |
| SN.PP (°) | SN to the palatal plane angle |
| SN.GOGN (°) | SN to Go-Gn angle |
| PP.MP (°) | Angle between the palatal plane (ANS/PNS) and the mandibular (Go/Gn) plane |
| FMA (°) | Frankfort horizontal to the mandibular plane angle |
| Gonial angle (°) | Ar-Go to Go-Gn angle |
| LAFH (mm) | Lower anterior face height: distance from ANS to menton |
| Dental relationship (mm) | |
| Overbite | Distance between the maxillary and mandibular incisor borders perpendicular to the functional occlusal plane |
| Maxillary mesiodistal angulations (°) | |
| Mx4.BOP | Long axis of the maxillary first premolar to the BOP |
| Mx5.BOP | Long axis of the maxillary second premolar to the BOP |
| Mx6.BOP | Long axis of the maxillary first molar to the BOP |
| Mx7.BOP | Long axis of the maxillary second molar to the BOP |
| Mx4.PP | Long axis of the maxillary first premolar to the ANS-PNS angle |
| Mx5.PP | Long axis of the maxillary second premolar to the ANS-PNS angle |
| Mx6.PP | Long axis of the maxillary first molar to the ANS-PNS angle |
| Mx7.PP | Long axis of the maxillary second molar to the ANS-PNS angle |
| Mandibular mesiodistal angulations (°) | |
| Md4.BOP | Long axis of the mandibular first premolar to the BOP |
| Md5.BOP | Long axis of the mandibular second premolar to the BOP |
| Md6.BOP | Long axis of the mandibular first molar to the BOP |
| Md7.BOP | Long axis of the mandibular second molar to the BOP |
| Md4.MP | Long axis of the mandibular first premolar to the mandibular plane (Go-Gn) angle |
| Md5.MP | Long axis of the mandibular second premolar to the Go-Gn angle |
| Md6.MP | Long axis of the mandibular first molar to the Go-Gn angle |
| Md7.MP | Long axis of the mandibular second molar to the Go-Gn angle |
| Interdental angulations (°) | |
| Mx4.Md4 | Long axes of the maxillary and mandibular first premolars |
| Mx5.Md5 | Long axes of the maxillary and mandibular second premolars |
| Mx6.Md6 | Long axes of the maxillary and mandibular first molars |
| Mx7.Md7 | Long axes of the maxillary and mandibular second molars |
These data were stored in a computer and analyzed with Dentofacial Planner software (version 7.0; Dentofacial Software, Toronto, Ontario, Canada), which corrected the image magnification factors of the x-rays.
The lateral headfilms obtained in the open-bite group were taken with various x-ray machines, which produced different magnification factors of the images, ranging from 6% to 10.94%. All lateral cephalograms in the normal occlusion group were taken with the same x-ray machine, which had a magnification factor of 6%.
To evaluate the intraexaminer errors, 14 radiographs were randomly selected, traced, digitized, and measured again by the same operator (V.L.) after a 30-day interval. The random errors were calculated according to Dahlberg’s formula (Se 2 = ∑d 2 /2n), where Se 2 is the error variance and d is the difference between 2 determinations of the same variable, and the systematic errors were calculated with dependent t tests, at P <0.05.
Statistical analyses
To assess normal distribution of the data in the sample, Kolmogorov-Smirnov tests were performed. All variables had a normal distribution in both groups.
We used t tests to evaluate the groups’ comparability regarding age, and the chi-square test was used to compare the groups regarding sex distribution.
Intergroup comparisons of all variables were performed with t tests.
The results were considered significant at P <0.05. All statistical analyses were performed with Statistica software (Statistica for Windows, version 10.0; StatSoft, Tulsa, Okla).
Results
No systematic errors were found, and the random errors were within acceptable limits, varying from 0.47° (ANB) to 3.99° (Mx7.BOP).
The 2 groups where comparable regarding age and sex distribution ( Tables II and III ).
| Variable | Group 1, open bite (n = 45) |
Group 2, normal occlusion (n = 45) |
P | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Age (y) | 13.95 | 1.89 | 13.83 | 0.95 | 0.700 |
| Group | Sex | ||
|---|---|---|---|
| Boys | Girls | Total | |
| Group 1, open bite | 20 | 25 | 45 |
| Group 2, normal occlusion | 23 | 22 | 45 |
| Total | 43 | 47 | 90 |
The open-bite group showed significantly more retruded mandibles, greater Class II skeletal relationships, and more upward inclinations of the palatal plane than did the normal occlusion group ( Table IV ). There were also significantly more accentuated vertical growth patterns and smaller overbites in the open-bite group.
| Variable | Group 1, open bite (n = 45) | Group 2, normal occlusion (n = 45) | P | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Maxillomandibular relationship (°) | |||||
| SNA | 81.88 | 6.09 | 81.76 | 3.65 | 0.911 |
| SNB | 77.16 | 5.17 | 79.32 | 3.01 | 0.017 ∗ |
| ANB | 4.71 | 2.90 | 2.44 | 1.92 | 0.000 ∗ |
| Growth pattern | |||||
| SN.PP (°) | 6.58 | 3.62 | 8.40 | 3.03 | 0.001 ∗ |
| SN.GoGn (°) | 39.52 | 6.64 | 32.38 | 4.72 | 0.000 ∗ |
| PP.MP (°) | 32.93 | 5.45 | 23.98 | 4.58 | 0.000 ∗ |
| FMA (°) | 33.68 | 5.15 | 28.32 | 4.61 | 0.000 ∗ |
| Gonial angle (°) | 129.26 | 5.57 | 125.84 | 6.74 | 0.010 ∗ |
| LAFH (mm) | 71.54 | 5.57 | 63.94 | 4.58 | 0.000 ∗ |
| Dental relationship (mm) | |||||
| Overbite | −2.68 | 2.05 | 3.04 | 1.10 | 0.000 ∗ |
| Maxillary mesiodistal angulations (°) | |||||
| Mx4.BOP | 75.47 | 5.04 | 79.23 | 4.34 | 0.000 ∗ |
| Mx5.BOP | 83.95 | 3.89 | 86.56 | 3.69 | 0.001 ∗ |
| Mx6.BOP | 90.78 | 4.72 | 89.94 | 4.28 | 0.378 |
| Mx7.BOP | 99.57 | 6.16 | 96.80 | 5.75 | 0.030 ∗ |
| Mx4.PP | 94.94 | 5.33 | 94.25 | 5.20 | 0.538 |
| Mx5.PP | 86.47 | 5.09 | 86.94 | 4.73 | 0.653 |
| Mx6.PP | 79.64 | 5.62 | 83.55 | 4.49 | 0.000 ∗ |
| Mx7.PP | 70.84 | 7.38 | 76.69 | 5.54 | 0.000 ∗ |
| Mandibular mesiodistal angulations (°) | |||||
| Md4.BOP | 76.65 | 5.74 | 82.95 | 4.21 | 0.000 ∗ |
| Md5.BOP | 78.46 | 5.43 | 84.05 | 4.11 | 0.000 ∗ |
| Md6.BOP | 81.37 | 4.82 | 82.22 | 4.20 | 0.377 |
| Md7.BOP | 76.56 | 5.29 | 78.07 | 5.18 | 0.174 |
| Md4.MP | 79.99 | 5.77 | 79.56 | 5.14 | 0.712 |
| Md5.MP | 78.18 | 4.97 | 78.47 | 5.19 | 0.786 |
| Md6.MP | 75.27 | 5.41 | 80.30 | 4.23 | 0.000 ∗ |
| Md7.MP | 80.08 | 5.74 | 84.45 | 4.48 | 0.000 ∗ |
| Interdental angulations (°) | |||||
| Mx4.Md4 | 152.13 | 6.93 | 162.20 | 6.21 | 0.000 ∗ |
| Mx5.Md5 | 162.40 | 6.66 | 170.61 | 5.10 | 0.000 ∗ |
| Mx6.Md6 | 171.97 | 5.31 | 172.08 | 3.81 | 0.914 |
| Mx7.Md7 | 175.96 | 7.00 | 174.88 | 4.21 | 0.376 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


