and Angela J. Yoon1
(1)
Columbia University College of Dental Medicine and Department of Pathology and Cell Biology, Columbia University Medical Center, New York, NY, USA
Pigmented lesions of the oral mucosa in children can be either exogenous or endogenous in origin. Examples of exogenous pigmentations include amalgam tattoo and pigmented hairy tongue. Endogenous pigmentations include focal or generalized melanosis and melanocytic nevi. Oral melanoma is exceedingly rare in children.
Medications can cause either exogenous or endogenous pigmentations. Exogenous pigmentation from medication results when the drug metabolite becomes deposited in the oral hard or soft tissue. An example of this is tetracycline staining. Endogenous pigmentation from medication results when the drug actually stimulates the production of melanin in oral mucosa. This type of medication-induced pigmentation might be seen in children with cancer who are receiving certain chemotherapeutic agents or in HIV positive children being treated with AZT.
Dependent on the type of pigmented lesion, focal pigmentations include amalgam tattoos, melanotic macules, and melanocytic nevi. Diffuse pigmentation includes physiologic pigmentation, pigmented hairy tongue, and medication-induced pigmentation.
The color also is variable depending on the source. In general, melanocytic lesions appear light to dark brown. Blue nevi appear gray-blue to bluish black. Exogenous pigmentations vary depending on the agent responsible. The most common exogenous pigmentation – the amalgam tattoo – appears grayish blue to black.
|
Pigmented lesions
|
|---|
|
Amalgam tattoo
|
|
Melanotic macule (focal melanosis)
|
|
Mucosal nevi
|
|
Physiologic (racial) pigmentation
|
6.1 Amalgam Tattoo
Clinical Appearance
Silver/gray, blue or black macule of the mucosa, often focal with either well defined, irregular, or defuse borders. Diagnosis is most often clinical based on appearance and history.
Etiology
Arise from iatrogenic implantation of amalgam particles or amalgam dust during the placement, polishing, or removal of amalgam fillings or apicoectomies.
Location
Any mucosal tissue, floor of mouth and gingival tissues adjacent to an amalgam restoration are common locations.
Differential Diagnosis
Melanotic macule, melanocytic nevus.
Treatment
Once diagnosis is established no treatment is needed.
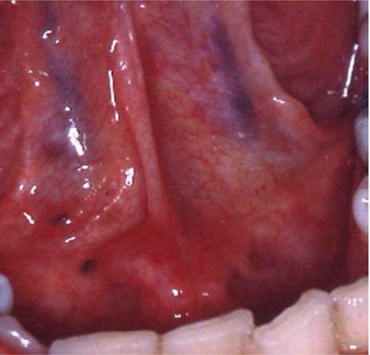
Fig. 6.1
Amalgam tattoo (2) of the floor of mouth. Patient had amalgam restorations on the occlusal surfaces of right and left mandibular first molars. Note the lingual veins for color comparison
Clinical Note
The child must have a history of amalgam restoration. With the advent of composite restorations, the prevalence of amalgam tattoos will likely decrease.
Depending on the size of the embedded particles, some amalgam tattoos can be confirmed by radiograph.

Fig. 6.2
Amalgam tattoo of the lingual tongue. This amalgam tattoo is large with irregular and diffuse borders (in contrast to Fig. 1). Patient had history of amalgam restorations of the occlusal surface and interproximal surfaces of the adjacent mandibular molar

Fig. 6.3
Amalgam tattoo of the posterior buccal mucosa. Patient had amalgam restorations on the occlusal surface of maxillary first molar


