Introduction
Orthodontic force duration can affect the severity of root resorption. The aim of this clinical study was to investigate the amounts of root resorption volumetrically after the application of controlled light and heavy forces in the buccal direction for 4, 8, and 12 weeks.
Methods
The sample consisted of 54 maxillary first premolars in 36 patients (mean age, 14.9 years; 21 girls, 15 boys) who required first premolar extractions as part of their orthodontic treatment. The teeth were allocated into 3 groups that varied in the duration of force application: 4, 8, or 12 weeks. The right or left first premolars were randomly selected to receive 2 levels of forces. A light buccally directed orthodontic force of 25 g was applied to the experimental tooth on 1 side, while a heavy orthodontic force of 225 g was applied on the contralateral premolar. At the end of the experimental period, the teeth were extracted and scanned with the microcomputed-tomography x-ray system. Resorption crater analysis was performed with specially designed software for direct volumetric measurements.
Results
Significant differences in the extent of root resorption were found between 4, 8, and 12 weeks of force application ( P <0.001), with substantially more severe resorption in the longer force duration groups. The light force produced significantly less root resorption than did the heavy force.
Conclusions
After 4, 8, or 12 weeks of buccally directed orthodontic forces applied on the maxillary first premolars, the volumes of root resorption craters were found to be related to the duration and the magnitude of the forces.
It has long been known that orthodontic tooth movement leads to external root resorption, after Ketcham reported the evidence of radiographic root resorption; however, the precise etiology remains unclear.
Becks and Marshall defined resorption as the destruction of formed tooth structure. Resorption of calcified dental tissue occurs when odontoclasts obtain access to the mineralized tissues by a breach in the formation cell layer covering the tissues. Root resorption is an undesirable effect during orthodontic movement, and it is believed to take place when local areas of the periodontal ligament are overcompressed. Therefore, root resorption is a concern for the orthodontic specialty, since it lessens the value of successful orthodontic treatment.
Many previous investigators have linked root resorption to various factors that might act as a single or multi-factorial cause, including type of orthodontic appliance, magnitude of applied force, duration of force application, type of tooth movement, amount of tooth movement, systemic factors, age of the patient, sex, nutrition, previous trauma, and ethnicity.
The magnitude of orthodontic force has been shown to be a primary factor in root resorption. Light forces have long been recommended to reduce adverse tissue reactions. However, Owman Moll et al found, in a histologic study, no significant difference in the frequency or severity of root resorption between groups receiving orthodontic forces of 50 and 200 g.
Significant correlations between orthodontically induced inflammatory root resorption (OIIRR) and treatment duration have been shown in several studies, although it has not been supported in a few studies. Kurol et al applied 50 cN of controlled continuous orthodontic force to 56 premolars. The experiment showed that the amount of root resorption increased with a longer period of force application. After 7 weeks, the tested teeth showed on average more than 20 times the resorbed root contour than did the control teeth. In a radiographic study by Mohandesan et al, the root-length reductions of the maxillary central incisors were 4.5% and 9.8% of the initial root lengths (0.77 and 1.67 mm), respectively, during 6 and 12 months of active treatment, whereas the corresponding root losses of the lateral incisors were on average 5.6% and 11.5% of the initial root lengths (0.88 and 1.79 mm), respectively. In an animal study, Maltha et al reported that the amount of OIIRR increased according to the period of force application. After 7 days of force application, root resorption was already present in some surfaces and progressing with time. After 14 to 17 weeks of tooth movement, the root resorption extended up to 94% of the observed root surfaces. On the other hand, a study of OIIRR in adult orthodontic patients supported the opposite opinion. The samples included 343 patients from 4 orthodontic practices. Using periapical radiographs of the maxillary anterior teeth and cephalograms, the authors concluded that treatment time was not associated with OIIRR.
The aim of this study was to compare the amounts of root resorption after the application of controlled light and heavy orthodontic forces for 4, 8, and 12 weeks.
Material and methods
The sample consisted of 54 maxillary first premolars from 36 patients (21 girls, 15 boys) who required the bilateral removal of these teeth as part of their orthodontic treatment. Their mean age was 14.9 years. Ethics approval was obtained from the Human Ethics Committee at the University of Sydney in Australia and Ondokuz Mayis University in Turkey before the investigation. All subjects completed written informed consent. The subject selection criteria were described previously. The 54 maxillary first premolars were allocated into 3 groups varying in duration of force application.
Group I consisted of 16 maxillary first premolars from 8 subjects and an experimental period of 4 weeks. This group was subdivided into 2 groups, each consisting of 8 premolars. Group Ia received a light force (25 g), and group Ib received a heavy force (225 g).
Group II consisted of 18 randomly selected right or left maxillary first premolars from 18 subjects with an experimental period of 8 weeks. The contralateral premolars were part of another study. This group was subdivided into 2 groups, each consisting of 9 premolars. Group IIa received a light force (25 g), and group IIb received a heavy force (225 g).
Group III consisted of 20 maxillary first premolars and 10 subjects with an experimental period of 12 weeks. This group was subdivided into 2 groups, each consisting of 10 premolars. Group IIIa received a light force (25 g), and group IIIb received a heavy force (225 g).
The subjects were bonded with 0.022-in SPEED brackets (Strite Industries, Cambridge, Ontario, Canada) on the maxillary first permanent molars and the experimental premolars. In the light-force groups (Ia, IIa, and IIIa), a light buccally directed orthodontic force of 25 g was applied on the maxillary first premolars by using 0.016-in beta-titanium alloy cantilever springs. In the heavy force groups (Ib, IIb, and IIIb), 225 g of buccally directed force was applied by using 0.017 × 0.025-in beta-titanium alloy cantilever springs. The force magnitudes were measured to the desired levels with a strain gauge (Dentaurum, Ispringen, Germany) ( Fig 1 ). To prevent occlusal interference of the experimental premolars and spring deformation, light-cured cement (Transbond Plus, 3M Unitek, Monrovia, Calif) was bonded onto the occlusal surfaces of the mandibular first permanent molars. The patients were checked every 4 weeks to ensure that the experimental appliances were in good condition.

After the force applications of 4, 8, and 12 weeks, the teeth were extracted with care to prevent surgical trauma to the root cementum. Upon removal, each tooth was immediately stored in an individual container of sterilized deionized water (Milli Q, Millipore, Bedford, Mass), which has been previously tested as a suitable storage medium. The tooth was then placed in an ultrasonic bath for 10 minutes to remove all traces of residual periodontal ligament and soft-tissue fragments. After the ultrasonic bath, the periodontal ligament was removed by a damp gauze swab with a rubbing motion, until all visible signs of it were gone. The tooth was then disinfected in 70% alcohol for 30 minutes and then bench dried at ambient room temperature (23°C ± 1°C).
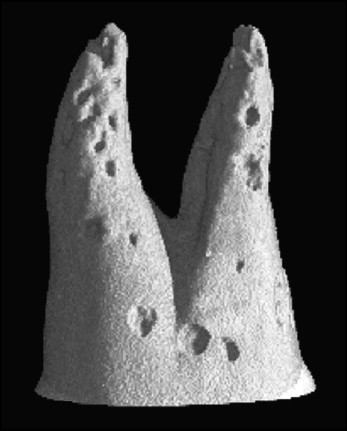
Each tooth was scanned separately 2 to 3 mm coronal to the cementoenamel junction ( Fig 2 ). This protocol was carried out with the same methodology as described in a previous study.
Statistical analysis
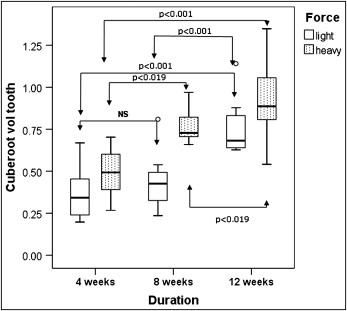
The amount of root resorption on each tooth was investigated by using univariate analysis of variance (ANOVA) with SPSS for Windows software (version 14, SPSS, Chicago, Ill). The factors used in the model were duration and force as fixed factors and subject (within group) as the random factor. Pairwise comparisons (with the Bonferroni adjustment for multiple comparisons) were used to compare the amount of root resorption at the 3 durations of force application. The significance level of each test was set at 5%. To satisfy the statistical assumptions necessary for these analyses (eg, normality of the residuals), the volumes of root resorption were transformed to the cube-root scale. Essentially, this process measures the amount of root resorption on a particular tooth not by the actual volume but by the radius of each hemispheric crater. This process allows a valid analysis, and the results can be expressed on the original (volume) scale. This approach was also used in previous studies.
Results
Highly significant differences among the 3 groups of force duration and the 2 groups of force magnitude were obtained ( P <0.001) ( Table I , Fig 3 ). The amount of root resorption produced from the different durations of force application was highest in the 12-week group followed by 8-week and 4-week groups, with means 0.75, 0.44, and 0.37 mm, respectively, for the light-force groups, and 0.92, 0.77, and 0.49 mm, respectively, for the heavy-force groups on the cube-root scale ( Table II ). Therefore, the longer the force duration and the heavier the force magnitude, the greater the amount of root resorption.
| Type III sum of squares | df | Mean square | F | Significance | |
|---|---|---|---|---|---|
| Intercept | |||||
| Hypothesis | 20.781 | 1 | 20.781 | 499.682 | <0.001 |
| Error | 1.305 | 31.387 | 0.042 | ||
| Force | |||||
| Hypothesis | 0.208 | 1 | 0.208 | 23.309 | <0.001 |
| Error | 0.152 | 17 | 0.009 | ||
| Duration | |||||
| Hypothesis | 1.480 | 2 | 0.740 | 17.609 | <0.001 |
| Error | 1.311 | 31.206 | 0.042 | ||
| Subject (duration) | |||||
| Hypothesis | 1.261 | 33 | 0.038 | 4.284 | 0.001 |
| Error | 0.152 | 17 | 0.009 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


