Tracheotomy is one of the most commonly performed procedures in critically ill patients. This article describes in particular the use of percutaneous dilatational tracheotomy. A brief history is included.
Airway access via tracheotomy is one of the most commonly performed procedures in critically ill patients. Despite being one of the oldest surgical procedures, first documented approximately 4000 years ago, it was not until the early 20th century that it is was deemed safe and viable when Jackson established clinical guidelines and proper surgical technique. Variations of the standard open tracheotomy have evolved over the last 50 years as technological advances and interest in minimally invasive techniques have grown. Since Ciaglia and colleagues introduced the percutaneous dilatational tracheotomy (PDT) in 1985; percutaneous tracheotomy (PCT) has become increasingly popular. In fact, PCT has gained widespread acceptance in many intensive care units (ICUs) and trauma centers as a viable alternative approach, and in some cases, it is the procedure of choice.
There are various types of PDT techniques available, the majority of which require puncture of the trachea with subsequent guide wire insertion. Three major modifications have occurred in the basic technique since Ciaglia’s initial report. First, the tracheal interspace for cannulation has been moved one or two levels caudal to the cricoid cartilage. Second, a single beveled curved dilator has replaced multiple sequential dilators. Third, the routine use of video fiberoptic bronchoscopy has been advocated to improve the safety of the procedure.
History of the procedure
Attempts at PCT began soon after Seldinger first described arterial line placement via catheter insertion over a guide wire. In 1955, Shelden and colleagues reported the first PCT attempt by guiding a cutting trocar into the trachea on a slotted needle. Unfortunately, the trocar used for this method caused multiple complications including fatalities from injury to adjacent vital structures. Since then, percutaneous airway access methods have improved, and various refinements to the technique have been reported.
Toye and Weinsten reported in 1969 on a technique in which they introduced a single tapered dilator with a recessed cutting blade inserted over a guiding catheter. The blade was designed to cut tissues placed under tension as the dilator was advanced into the trachea.
In 1985, Ciaglia and colleagues described the PDT. In their method, a guide wire was introduced into the airway through a needle. This was followed by serial dilations with sequentially larger dilators.
In 1989, Schachner and colleagues reported the Rapitrach method, which employed a dilating forceps device containing a beveled metal cone-shaped tip designed to be advanced with pressure over a wire into the trachea.
Griggs and colleagues in 1990 reported the guide wire dilating forceps method similar to the Rapitrach method with the exception that the tip of the instrument did not have a cutting edge.
In 1997, Fantoni and Ripamonti described the translaryngeal tracheotomy, which employed a specially designed cannula used to dilate the trachea in a retrograde manner.
Byhahn and colleagues in 2000 introduced the Ciaglia Blue Rhino, which was a modified version of the previously described Ciaglia technique. They modified the dilator so a hydrophilically coated curved dilator, the Blue Rhino, was used to dilate the stoma in a single step rather than multiple steps. They stated that the risk of posterior tracheal wall injury and intraoperative bleeding was reduced. Additionally, the technique minimized the risk of adverse oxygen desaturation during repeated airway obstruction caused by use of multiple dilators. The use of bronchoscopic guidance was advocated for monitoring the procedure .
In 2002, Frova and Quintel introduced a new variation on PCT called the PercuTwist technique. This technique features a single-step dilator with a self-tapping screw (PercuTwist, Rusch, Kernen, Germany) used to achieve a controlled rotating dilation of the airway. In their preliminary study, no significant bleeding or other relevant procedure related complications were found.
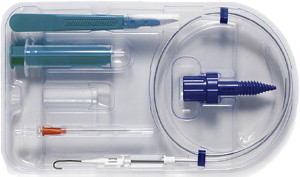
Percutwist set
In 2008, Gromann and colleagues introduced balloon dilatational tracheotomy . The balloon mainly exerts radial force to widen the tracheotomy site, which theoretically aims to reduce typical complications such as fracture of the tracheal cartilage rings or injuries to the posterior tracheal wall.
Indications
In general terms, indications for percutaneous tracheotomy are the same as those for standard open tracheotomy. The most common indication for the procedure is a need for airway access for prolonged mechanical ventilation. The Council on Critical Care of the American College of Chest Physicians gives recommendations for tracheotomy for those patients expected to require mechanical ventilation for longer than 7 days.
Indications
In general terms, indications for percutaneous tracheotomy are the same as those for standard open tracheotomy. The most common indication for the procedure is a need for airway access for prolonged mechanical ventilation. The Council on Critical Care of the American College of Chest Physicians gives recommendations for tracheotomy for those patients expected to require mechanical ventilation for longer than 7 days.
Contraindications
There has been much debate over what constitutes absolute and relative contraindications for the procedure. In their recent review, Al Asari and Hijazi described them. Specifically, contraindications are listed in Box 1 .
-
Absolute contraindications
-
Patient age younger than 8
-
Necessity of emergency airway access because of acute respiratory compromise
-
Gross distortion of the neck anatomy due to:
-
Hematoma
-
Tumor
-
Thyromegaly
-
High innominate artery
-
-
Relative contraindications
-
Patient obesity resulting in loss of palpable anatomic landmarks
-
Refractory bleeding diatheses
-
Prothrombin time or activated prothrombin time greater than 1.5 times normal
-
Platelet count less than 50,000/μL
-
Bleeding time greater than 10 minutes
-
Need for positive end–expiratory pressure (PEEP) greater than 20 cm water
-
Evidence of soft tissue neck infection involving planned surgical site
-
Most publications consider cervical injury, pediatric age, coagulopathy, and emergency airway access as absolute contraindications, whereas short stature, thick neck, or obesity are relative contraindications. Several reports, however, recently have emerged specifically addressing the safety and feasibility of performing PCT in patients with previously described contraindications for the procedure .
For instance, in patients with inability to extend the neck due to lack of cervical spine clearance, the PCT complication rate has been reported to be 7.1% . PCT also has been reported to be a safe method of airway access in patients who have undergone anterior cervical spine fusions .
Byhahn and colleagues studied the safety of percutaneous tracheotomy in 73 obese patients (body mass index 27.5 kg/m 2 ) in a cohort of 474 adults. The overall complication rate was 43.8% (n = 32) in the obese group compared with 18.2% (n = 73) in the control group. Obese patients had a 2.7-fold increased risk for perioperative complications and a 4.9-fold increased risk for serious complications .
Bronchoscopically guided PDT in patients with low platelet counts who are platelet transfused before the procedure, or patients who have their heparin therapy temporarily suspended during the procedure, are reported to have low complication rates .
The impact of bronchoscopically guided PDT on oxygenation in patients with hypoxic respiratory failure requiring high PEEP was studied recently. The results suggested high PEEP did not jeopardize oxygenation 1 hour and 24 hours after the procedure, and PDT may be performed safely in patients with acute respiratory distress syndrome with high PEEP requirements .
Although in the earlier reports, most authors considered PCT to be contraindicated in emergency airway management, more recent evidence supports the feasibility and safety of emergency PCT even in these settings .
Preoperative details
Equipment
Necessary equipment includes
-
PDT kit (Cook Critical Care Incorporated, Bloomington, IN, USA): 22-gauge needle and syringe; 11-F short punch dilator; 1.32-mm guide wire; 8-F guiding catheter; 18-F, 21-F, 24-F, 28-F, 32-F, 36-F, and 38-F dilators; Shiley size 8 double-cannula tracheotomy tube; fiberoptic bronchoscope
-
GWDF kit (Sims Portex, Hythe, UK): 14-gauge needle and syringe, guide wire (J-tipped Seldinger wire type), scalpel, Howard-Kelly forceps modified to produce a pair of GWDF, Shiley size 8 double-cannula tracheotomy tube with curved obturator, fiberoptic bronchoscope
-
Rapitrach kit (Fresenius, Runcorn, Cheshire, UK): 12-gauge needle and syringe, short guide wire, scalpel, Rapitrach PCT dilator, standard Portex 8-mm tracheotomy tube with curved obturator, fiberoptic bronchoscope
-
Ciaglia Blue Rhino kit (Cook Critical Care Incorporated, Bloomington, IN, USA): 14-gauge catheter introducer needle and syringe, guide wire (J-tipped Seldinger wire type), guiding catheter, introducer dilator, loading dilators, single tapering Blue Rhino dilator, size 8 Shiley tracheotomy tube with curved obturator; fiberoptic bronchoscope.
Preparation
Proper preparation requires
-
Intravenous sedation and short-acting paralysis
-
Oxygenation with 100% oxygen before and throughout the procedure (as opposed to the open procedure, where the oxygen is reduced if the electrocautery is used)
-
Proper positioning of the patient with neck extension if needed, assuming there are no contraindications
-
Cleaning the endotracheal (ET) tube with suctioning and lavage if needed.
Percutaneous dilatational tracheotomy techniques
The neck is prepared and draped in the usual sterile fashion. Patients with a short neck or low cricoid cartilage are extended with a shoulder roll. The cricoid cartilage is identified. The skin can be injected with 1% lidocaine with 1:100,000 epinephrine. A 1.5- to 2-cm vertical skin incision is made at the level of the second and third tracheal rings. Then, blunt dissection of the midline may be performed. A 16-gauge needle is inserted between the first and second or the second and third tracheal rings. When air is aspirated into the syringe, or when the position of the needle is verified by bronchoscopy, the guide wire is introduced. The needle is removed, and the guide wire is left in place. The dilators are introduced in a sequential manner from small to large diameter. The tracheotomy tube is placed over the appropriate size introducer and the assembly passed over the guide wire. The tracheotomy tube then is introduced, and the cuff is inflated. The guide wire and introducer are removed, and the breathing circuit is connected. The ET tube is removed after proper placement of tracheotomy tube is confirmed by returning end–tidal CO 2 or visual confirmation via transendotracheal tube videobronchoscopy.
In all of the techniques in the following sections, the basic initial and concluding steps of the tracheotomy procedures are similar to the aforementioned technique. Therefore only the differences in techniques will be emphasized.
Guide Wire Dilating Forceps Technique
After initial preparation, a 14-gauge intravenous needle with saline-filled syringe is inserted in the midline of the incision. When proper placement is confirmed by visualization of air bubbles in the syringe, the outer plastic cannula is advanced into the lumen of the trachea, and the needle is removed. A J-tipped Seldinger wire is introduced into the trachea, and the plastic cannula is removed. The tip of the Seldinger wire is passed through the closed locked guide wire dilating forceps (GWDF). The forceps are advanced through the soft tissues of the neck until resistance is felt. The GWDF are released and opened to dilate the soft tissues anterior to the trachea, and the forceps then are closed, locked, and reinserted over the wire into the trachea. A slight loss of resistance occurs as the tracheal membrane is pierced. To prepare the stoma of the tracheotomy, the GWDF are opened to the same diameter as during that done with dilation of the soft tissues. A tracheotomy tube with obturator is inserted over the guide wire and advanced into the trachea. The obturator and guide wire are removed.
Rapitrach Technique
With this technique, the subcutaneous layers are dissected bluntly with a pair of forceps until the tracheal rings can be palpated with a finger. A 12-gauge needle is inserted into the trachea. In this technique, the Rapitrach dilator is introduced into the trachea over a guide wire. The dilator is opened when its tip lies in the trachea. A tracheotomy tube with obturator is inserted through the dilator jaws into the trachea.
Ciaglia Blue Rhino Technique
A 1 cm skin incision is made vertically in the low central neck between the inferior aspect of the cricoid cartilage and the suprasternal notch. A 16-gauge angiocatheter is inserted between the first and second or the second and third tracheal rings. When air is aspirated into the saline-filled syringe or when the position of the needle is verified by bronchoscopy ( Fig. 1 A), the needle is removed, leaving the plastic catheter in place (see Fig. 1 B). The guide wire then is introduced through the catheter (see Fig. 1 C). The catheter is removed leaving the guide wire in the distal trachea (see Fig. 1 D). Next, a small dilator is advanced over the guide wire to dilate the skin and anterior tracheal wall. This small dilator is removed, thus allowing the insertion of a more rigid plastic sheath that prevents kinking of the guide wire during the final dilation step (see Fig. 1 E). Then, the Blue Rhino single tapering dilator (white in color) is introduced over the sheath/sheath combination until the stoma is dilated to the marked diameter (36-F) (see Fig. 1 F). Once proper dilation is achieved, a cuffed tracheotomy tube, previously assembled over one of the three appropriately sized introducers, is advanced over the sheath/sheath until the cannula is in place within the tracheal lumen (see Fig. 1 G). The introducer and sheath/sheath are removed; the cuff is inflated, and the breathing circuit is connected (see Fig. 1 H). Bronchoscopic guidance of the needle and the guide wire insertion is strongly recommended with this technique. Bronchoscopic guidance during PCT appears to be the most significant contributing factor responsible for potential hypercarbia developing during the procedure. Therefore, bronchoscopic guidance should be limited to the initial dilatation steps only. The prepackaged set is shown in Fig. 2 .


