Introduction
The purposes of this study were to investigate the patterns of tooth agenesis (oligodontia and nonoligodontia), maxillary canine impaction, and tooth transposition in subjects with Down syndrome and to determine whether congenital heart disease and hypothyroidism are parameters in tooth agenesis.
Methods
The study included 114 patients with Down syndrome. The data were quantified by using standardized records, clinical examinations, panoramic radiographs, and solo roentgenograms. The subjects were differentiated into oligodontia (6 or more teeth missing) and nonoligodontia (5 or fewer teeth missing).
Results
In these patients with Down syndrome, 59.6% had missing teeth. Those in the nonoligodontia group showed a tendency toward a negative correlation between congenital heart disease and agenesis ( P = 0.093; odds ratio = 0.49) but a slight positive correlation between hypothyroidism and agenesis ( P = 0.060; odds ratio = 3.71). In the oligodontia group, there was a quantitatively and qualitatively different pattern, indicating another phenotype. When both mandibular central incisors were missing, there was a remarkable chance for oligodontia ( P = 0.001; odds ratio = 38.8). In the mandible, symmetrical agenesis of the canines and lateral incisors was more frequent in the nonoligodontia group.
Conclusions
The oligodontia (with a different phenotype) and nonoligodontia groups had different patterns of agenesis. Maxillary canine impaction was not related to absence of the lateral incisors. Absence of both mandibular central incisors was a high predictor for oligodontia. Congenital heart disease and hypothyroidism are parameters involved in tooth agenesis.
Recently, mouse models showed that the Down syndrome (DS) critical region (DSCR1) on chromosome 21 is not the cause of the expression of craniofacial or cardiac development. Rather, the occurrence of these diseases is greatly increased by trisomy 21 only indirectly. It can be hypothesized that a threshold effect of total transcript and protein level must be reached for certain DS-related phenotypes to appear. There is now a need for more fundamental knowledge of phenotypic details. Discriminating between dental agenesis in oligodontia and nonoligodontia might help to acquire new insights.
Some aspects of DS phenotype are congenital: cardiac anomalies (40%-50%), small skull (100%), and dental agenesis (also known as hypodontia, 50% to 60%). Congenital cardiac anomalies are corrected with surgery during infancy. Congenital hypothyroidism is traced by neonatal screening, and often thyroid treatment is recommended. Hypodontia in patients with DS has been studied extensively, and its prevalence varies between populations in different countries. Treatment planning for the developing dentition is still deficient. However, hypodontia and specifically oligodontia merit treatment. Oligodontia is the congenital absence of 6 or more permanent teeth, excluding the third molars. Oligodontia has been reported, but no specific pattern has been described. Often it remains hidden in the overall data. Certain aspects of DS are manifested more prominently in childhood, such as growth retardation: underdevelopment of the midface subsequently resulting in malocclusion and delayed transition to the permanent dentition. Specific dental features are microdontia, altered crown morphology and shape, thinner enamel and dentin, taurodontism, and tooth transpositions. None of these dental features is unique to people with DS. They occur also in the normal population, but the frequency in people with DS is higher. Maxillary canine impaction is considered an associated phenomenon and is supposed to coincide with the absence of, or peg-shaped, maxillary lateral incisors, a condition often seen in patients with DS.
In addition to functional and esthetic problems, a disadvantage of congenital hypodontia is that there is less development of alveolar bone, resulting in decreased maxillary length and bone height. The latter factor makes patients with DS more vulnerable to loss of teeth from periodontal disease. Regular roentgen screening at 6, 9, 12, and 15 years of age is recommended. This provides information about hypodontia, impaction of teeth, stage of eruption, and development of the typically growing jaws. Guiding impacted teeth to the right positions might prevent malocclusion and lead to optimal bone height. Important for orthodontic treatment is that stature growth is retarded during childhood in patients with DS; the adolescent period is shorter, and maturation of the bones takes place around 15 to 17 years of age.
The goals of this study were (1) to investigate the patterns of dental agenesis in oligodontia and nonoligodontia, maxillary canine impaction and tooth transposition; (2) to determine whether congenital heart diseases and hypothyroidism are parameters involved in tooth agenesis; and (3) to raise awareness of the consequences of these aspects of the developing dentitions in patients with DS.
Material and methods
The sample involved 126 subjects with DS, all referred to the Centre for Special Care Dentistry, CBT Rijnmond, in Rotterdam, The Netherlands, by general practitioners. About 50% of the patients had roentgenograms taken under general anesthesia. Twelve patients were eliminated because taking roentgenograms was impossible; 114 subjects remained for data analysis (47 female, 67 male). The age range was 9.5 to 23.9 years (mean, 15.9 years; SD, 4 years). Patients aged 9 years and older were included in this study because calcification can be late in those with hypodontia. From each subject, a standardized record was obtained, including a detailed clinical examination. Presence or absence of heart disease and hypothyroidism was recorded. Panoramic radiographs were taken, and written parental informed consent was obtained. If this was not possible, a standardized roentgen set was made. Third molars were not included. Permanent teeth that were hypoplastic or radiographically observed but not yet erupted were considered present. In addition to agenesis, maxillary canine and first premolar transpositions, and impaction of canines were determined.
Statistical analysis
The FDI numbering system was used. Absent teeth were registered by tooth number. In addition, the tooth agenesis code (TAC) was calculated. With the TAC method, it is easy to represent combinations of tooth agenesis per quadrant; especially, the combination TAC values expresses the severity of the hypodontia per quadrant and gives valuable information to enable a rapid estimate for treatment planning ( Table ). However, the TAC obscures the symmetry of absent teeth between quadrants. Symmetric absence of teeth can be better represented by the percentage of agenesis by tooth type for the oligodontia and the nonoligodontia groups ( Figs 1 and 2 ). For descriptive statistics, cross tables and histograms were made. To test for relationships between dichotomous variables, the Fisher exact test was used. To explain the chance of a patient having oligodontia, or being without oligodontia (with some agenesis), logistic regression was used. Also, logistic regression was applied for the relationships between agenetic teeth and congenital heart disease and retarded thyroid function. To compare the number of missing teeth between jaws or quadrants, the Wilcoxon signed rank test was used. To compare the numbers of missing teeth between groups, the Mann Whitney U test was applied with SPSS statistical software (version 16, SPSS, Chicago, Ill).
| Tooth | Value |
|---|---|
| Central incisor | 1 |
| Lateral incisor | 2 |
| Canine | 4 |
| First premolar | 8 |
| Second premolar | 16 |
| First molar | 32 |
| Second molar | 64 |
| Third molar | 128 |
Results
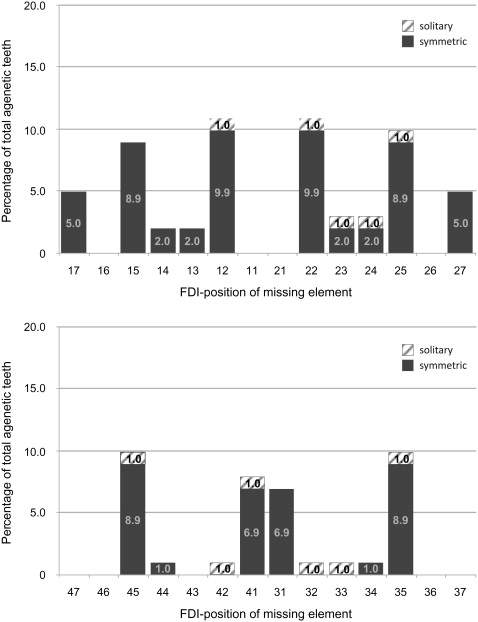
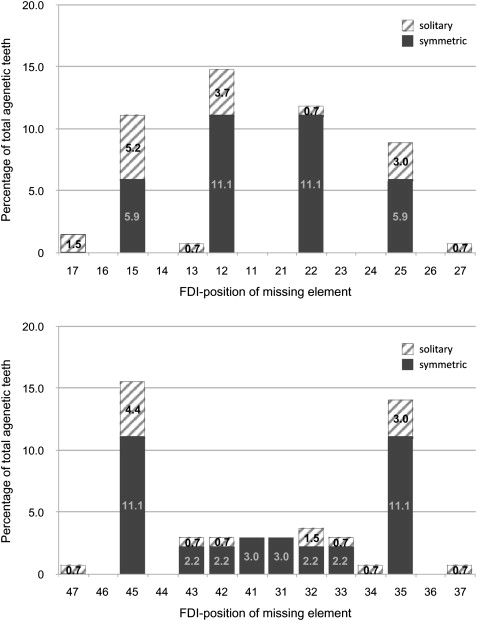
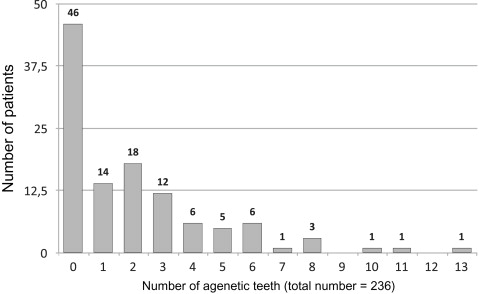
The prevalence of agenetic teeth in our subjects (n = 114) is shown in Figure 3 . A total of 236 teeth were missing, from 0 to 13 per patient (median, 1; quartiles, 0 and 3 missing teeth). Of the DS patients, 59.6% had at least 1 agenetic tooth. Figures 1 and 2 show the agenesis by tooth type as percentages of absent teeth in both jaws for the oligodontia (n = 13) and nonoligodontia (n = 101) groups. In the nonoligodontia group, 33 patients had congenital heart disease, with a tendency toward a negative correlation with agenetic teeth ( P = 0.093; odds ratio [OR], 0.49; 95% CI, 0.21-1.13). A tendency toward a positive correlation was observed between retarded thyroid function (13 patients) and agenetic teeth ( P = 0.060; OR, 3.71; 95% CI, 0.95-14.60). In the oligodontia group, there was no significant negative correlation between congenital heart disease (4 patients) and agenetic teeth, because of the small group (data not shown). In these 13 patients, no retarded thyroid function was seen. Impaction of 1 or 2 maxillary canines was seen in 13 patients in the group of 101 nonoligodontia patients. No impaction was seen in the oligodontia group. No relationship was found between this type of impaction and the absence of 1 or 2 maxillary lateral incisors ( P = 0.75).
The 13 oligodontia patients with DS (8 male, 5 female) were responsible for 101 agenetic teeth, ranging from 6 to 13 per patient (median, 7; quartiles, 6 and 9). In this group, there was a significant difference between the numbers of missing teeth in the maxilla (61; range, 2-8) and the mandible (40; range, 2-7; P = 0.025). There was no statistically significant difference in the number of absent teeth between the right and left sides of the face (maxilla plus mandible), the maxillary right and left quadrants, and the mandibular left and right quadrants ( P = 0.453, 0.180, and 1.00, respectively). No impaction of canines was seen.
The nonoligodontia group contained 101 patients (59 male, 42 female). They were responsible for 135 agenetic teeth, ranging from 0 to 5 per patient (median, 1; quartiles, 0 and 3). There was no statistically significant difference in the number of agenetic teeth between the sexes ( P = 0.721). No significant differences were seen in the numbers of absent teeth between the 2 jaws ( P = 0.755), between left and right sides of the face ( P = 0.128, or between the mandibular quadrants ( P = 1.00). However, there was a statistically significant difference between the maxillary right (38 missing teeth) and left (29 missing teeth) quadrants ( P = 0.05). When tooth numbers 31 and 41 were both agenetic in a child with DS, a positive relationship was obtained with oligodontia ( P = 0.001; OR, 38.8; 95% CI, 8.66-173.79). This relationship was not seen for the combination of teeth 32 and 42 ( P = 0.228; OR, 0.52; 95% CI, 2.88-16.04).
In the group with oligodontia. the most striking feature was that symmetric absence of teeth—absence in left-right symmetrical pairs—was more prevalent than solitary absence ( Fig 1 ). Of the 101 agenetic teeth, only 10.9% were solitarily absent. The maxillary lateral incisors were most often symmetrically absent, closely followed by the second premolars in both jaws. The mandibular central incisors followed next and then the maxillary second molars. Whereas symmetric absence of the maxillary canines was found, this was not the case in the mandible. In the maxilla, combination TAC 18 (27%) and 82 (23.1%) were the most common patterns ( Table ). TAC 18 represents a situation where the second premolar and the lateral incisor in the same quadrant are both absent; when the maxillary second molar is also absent, it is TAC 82. In the mandible, combination TAC 17 (26.9%) was found (absence of the second premolars and the central incisor). In the nonoligodontia group also, there was a pattern of symmetrical absence ( Fig 2 ). The frequency of missing maxillary lateral incisors was higher, followed by the mandibular second premolars and the maxillary second premolars. Notable was the general absence of combination TAC scores; only TAC 18 was found more than once (6 times) in the maxillary right quadrant. In the mandible, combination TACs were completely absent.
Three patients had transpositions of a canine and first premolar, and 1 patient had fusion of the first and second premolars, all in the maxilla. The nonoligodontia group had no symmetric absence of maxillary first premolars and canines. In contrast, symmetrical absences of the mandibular canines and lateral incisors were found at higher frequencies than in the oligidontia group. In the nonoligodontia group, solitary absence of teeth (21 times in the maxilla and 15 times in the mandible) was more prevalent than in the oligodontia group.
Results
The prevalence of agenetic teeth in our subjects (n = 114) is shown in Figure 3 . A total of 236 teeth were missing, from 0 to 13 per patient (median, 1; quartiles, 0 and 3 missing teeth). Of the DS patients, 59.6% had at least 1 agenetic tooth. Figures 1 and 2 show the agenesis by tooth type as percentages of absent teeth in both jaws for the oligodontia (n = 13) and nonoligodontia (n = 101) groups. In the nonoligodontia group, 33 patients had congenital heart disease, with a tendency toward a negative correlation with agenetic teeth ( P = 0.093; odds ratio [OR], 0.49; 95% CI, 0.21-1.13). A tendency toward a positive correlation was observed between retarded thyroid function (13 patients) and agenetic teeth ( P = 0.060; OR, 3.71; 95% CI, 0.95-14.60). In the oligodontia group, there was no significant negative correlation between congenital heart disease (4 patients) and agenetic teeth, because of the small group (data not shown). In these 13 patients, no retarded thyroid function was seen. Impaction of 1 or 2 maxillary canines was seen in 13 patients in the group of 101 nonoligodontia patients. No impaction was seen in the oligodontia group. No relationship was found between this type of impaction and the absence of 1 or 2 maxillary lateral incisors ( P = 0.75).
The 13 oligodontia patients with DS (8 male, 5 female) were responsible for 101 agenetic teeth, ranging from 6 to 13 per patient (median, 7; quartiles, 6 and 9). In this group, there was a significant difference between the numbers of missing teeth in the maxilla (61; range, 2-8) and the mandible (40; range, 2-7; P = 0.025). There was no statistically significant difference in the number of absent teeth between the right and left sides of the face (maxilla plus mandible), the maxillary right and left quadrants, and the mandibular left and right quadrants ( P = 0.453, 0.180, and 1.00, respectively). No impaction of canines was seen.
The nonoligodontia group contained 101 patients (59 male, 42 female). They were responsible for 135 agenetic teeth, ranging from 0 to 5 per patient (median, 1; quartiles, 0 and 3). There was no statistically significant difference in the number of agenetic teeth between the sexes ( P = 0.721). No significant differences were seen in the numbers of absent teeth between the 2 jaws ( P = 0.755), between left and right sides of the face ( P = 0.128, or between the mandibular quadrants ( P = 1.00). However, there was a statistically significant difference between the maxillary right (38 missing teeth) and left (29 missing teeth) quadrants ( P = 0.05). When tooth numbers 31 and 41 were both agenetic in a child with DS, a positive relationship was obtained with oligodontia ( P = 0.001; OR, 38.8; 95% CI, 8.66-173.79). This relationship was not seen for the combination of teeth 32 and 42 ( P = 0.228; OR, 0.52; 95% CI, 2.88-16.04).
In the group with oligodontia. the most striking feature was that symmetric absence of teeth—absence in left-right symmetrical pairs—was more prevalent than solitary absence ( Fig 1 ). Of the 101 agenetic teeth, only 10.9% were solitarily absent. The maxillary lateral incisors were most often symmetrically absent, closely followed by the second premolars in both jaws. The mandibular central incisors followed next and then the maxillary second molars. Whereas symmetric absence of the maxillary canines was found, this was not the case in the mandible. In the maxilla, combination TAC 18 (27%) and 82 (23.1%) were the most common patterns ( Table ). TAC 18 represents a situation where the second premolar and the lateral incisor in the same quadrant are both absent; when the maxillary second molar is also absent, it is TAC 82. In the mandible, combination TAC 17 (26.9%) was found (absence of the second premolars and the central incisor). In the nonoligodontia group also, there was a pattern of symmetrical absence ( Fig 2 ). The frequency of missing maxillary lateral incisors was higher, followed by the mandibular second premolars and the maxillary second premolars. Notable was the general absence of combination TAC scores; only TAC 18 was found more than once (6 times) in the maxillary right quadrant. In the mandible, combination TACs were completely absent.
Three patients had transpositions of a canine and first premolar, and 1 patient had fusion of the first and second premolars, all in the maxilla. The nonoligodontia group had no symmetric absence of maxillary first premolars and canines. In contrast, symmetrical absences of the mandibular canines and lateral incisors were found at higher frequencies than in the oligidontia group. In the nonoligodontia group, solitary absence of teeth (21 times in the maxilla and 15 times in the mandible) was more prevalent than in the oligodontia group.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


