Introduction
The effects of Invisalign clear aligner treatment with and without Dental Monitoring (DM) were compared for treatment duration, number of appointments, refinements and refinement aligners, and accuracy of Invisalign in achieving predicted tooth positions (aligner tracking). The null hypothesis was that there are no differences between Invisalign with and without DM in these parameters.
Methods
A sample of 90 consecutively treated Invisalign patients (45 control, 45 DM) fitted the inclusion and exclusion criteria. Treatment duration, number of refinements, number of refinement aligners, time to first refinement, number of appointments, number of emergency visits, and accuracy of predicted tooth movement were observed for differences.
Results
The 2 groups were homogeneous ( P >0.05) for sample size, age, gender, Angle classification, maxillary and mandibular irregularity index, and the number of initial aligners. There was a significant ( P = 0.001) reduction in the number of appointments by 3.5 visits (33.1%) in the DM group. There was also a significant ( P = 0.001) reduction in the time to the first refinement (1.7 months) in the DM group. Compared with Invisalign predicted tooth positions, actual tooth positions were statistically ( P <0.05) more accurate for the DM group for the maxillary anterior dentition in rotational movements and mandibular anterior dentition for buccal-lingual linear movement. Invisalign therapy without DM was closer to predicted tooth positions for the maxillary posterior dentition for the tip. None of these differences surpassed the clinically significant thresholds (>0.5 mm or >2°); however, the DM group achieved this in 1.7 fewer months.
Conclusions
DM with Invisalign therapy resulted in a reduced number of appointments by 3.5 visits (33.1%). The DM group also achieved a clinically similar accuracy in obtaining predicted tooth movements compared with the control group in 1.7 fewer months, indicating improved aligner tracking in the DM group.
Highlights
- •
Dental Monitoring reduced the number of in-office visits by 3.5 visits (33.1%).
- •
Duration to the first refinement was 1.69 months less in the Dental Monitoring group.
- •
Differences in the accuracy of achieving predicted tooth movement was insignificant.
The history of orthodontics is replete with the drive for greater treatment and chairside efficiency. , Evolution from banding to bracketing each tooth, the development of the straight wire appliance and nickel-titanium wires, and arguably self-ligating brackets and customized appliances have all substantially improved treatment and chair-time efficiency.
Treatment efficiency can be attributed foremost to an accurate diagnosis, competent treatment plan, and efficient biomechanics. Over the past 2 decades, research in improving orthodontic treatment efficiency has focused primarily on the biological aspect of accelerating tooth movement with corticotomies, periodontal accelerated osteogenic orthodontics (PAOO), , photobiomodulation, vibration therapy, and low-level laser therapy being the most popular. Less emphasis has been placed on other aspects of improving treatment efficiency, specifically increasing the frequency of patient monitoring, because of the associated clinical and financial drawbacks of increasing the number of appointments. Contrary to popular practice, there is some evidence indicating that shorter intervals between appointments reduce treatment times. , Chairside appointment schedules are planned to be optimally coordinated with the biological response to forces applied, given the patient’s periodontal condition. Standardized schedules can range from 7-day changes for aligner patients, 2-week appointments for accelerated orthodontic patients, and 4-to-8-week intervals for traditional orthodontic patients. The goal of teleorthodontics is to permit frequent, proactive remote monitoring, allowing for customized appointment frequency on the basis of the need for in-office visits and shorter treatment durations because of improved patient compliance and early interception of problems.
At the forefront of teleorthodontic technology is Dental Monitoring (DM). This novel technology allows patients to scan and capture their dentition using a smartphone and allows the orthodontist to review their progress remotely. DM consists of 3 integrated platforms: a mobile application for the patient, a patented movement-tracking algorithm, and a web-based doctor dashboard in which updates on the patient’s progress are received. Advocates of DM indicate a reduction in tracking problems, refinements, and treatment times, while at the same time reducing the number of office visits and increasing patient convenience.
DM is a new orthodontic concept, and only 4 studies have been published to date. Hansa et al reported a positive patient perception of DM and a significant reduction in the number of appointments. However, this pilot study was based on short term data and did not encompass the entirety of treatment. Moylan et al compared DM and plaster cast measurements of intermolar and intercanine widths on patients undergoing rapid maxillary expansion (RME) and found them clinically equivalent. Kuriakose et al also studied and verified the accuracy of DM on patients undergoing RME by comparing intermolar width measurements obtained by DM, intraoral examination, and digital models. In addition, they found that DM could correctly identify the correction of posterior crossbites remotely. Morris et al tested the accuracy of the digital models generated by DM in both photograph and video modes compared with digital models obtained from an intraoral scanner. They used 10 typodonts and simulated treatment using 10 Invisalign aligners and performed DM and intraoral scans at each stage. They examined the global deviations and concluded that there were no clinically significant differences between the DM and intraoral scans. An unpublished thesis by Ohanesian has similarly demonstrated a high level of accuracy when comparing measurements from DM scans to those obtained by an intraoral scanner on patients undergoing comprehensive orthodontic treatment.
Lacking investigation are the clinical implications and performance of DM with Invisalign treatment. The present investigation aimed to compare the effects of Invisalign with and without DM on the following parameters: treatment duration, number of appointments, number of refinements, total number of refinement aligners, time to initial refinement, number of emergency and/or unscheduled visits, and accuracy of Invisalign in achieving predicted tooth positions (aligner tracking).
Material and methods
Approval for this retrospective study was granted by the Institutional Review Board at the European University College (approval no. EUC-IRB-19.01.15). A power analysis using the number of appointments as the primary outcome was performed on the basis of the results of Hansa et al. Using an alpha of 0.05 and 80% power, it was determined a total sample size of 48 was required. However, to obtain adequate power for determining true differences in treatment duration and the other objectives with unknown or smaller effect sizes, a larger sample was required. Hence, a total of 115 (56 control, 59 DM) consecutively treated Invisalign patients were initially selected, of which 45 control patients and 45 DM patients met the following inclusion criteria: (1) treatment with Invisalign aligners, (2) between 15 and 50 initial aligners, (3) treatment with the default amounts of tooth movement in each aligner stage, (4) nonextraction treatment, and (5) a complete permanent dentition anterior to second molars. Patients were excluded from the study on the basis of the following exclusion criteria: (1) treatment encompassing orthognathic surgery, (2) combination treatment with fixed appliances or other auxiliary appliances, and (3) the presence of dental prostheses.
Treatment was provided by a single, experienced Invisalign provider orthodontist (V.K.) in a private practice setting. All patients were offered DM at the start of their treatment, with the control group scheduled for appointments at approximately 6-to-8-week intervals, and the DM group scheduled generally every 16 weeks. The control group changed aligners every 7 days, as per the standard protocol. The DM group was also recommended to change aligners every 7 days; however, this recommendation was dynamic as the DM software instructed the patient whether to proceed with the next aligner or continue with the same aligner.
The pretreatment data recorded were age, gender, Angle classification, maxillary and mandibular irregularity index, and number of initial aligners. In addition, each patient-subject was observed for treatment duration (in months), number of refinements, number of refinement aligners, time to first refinement, number of appointments, and number of emergency and/or unscheduled visits.
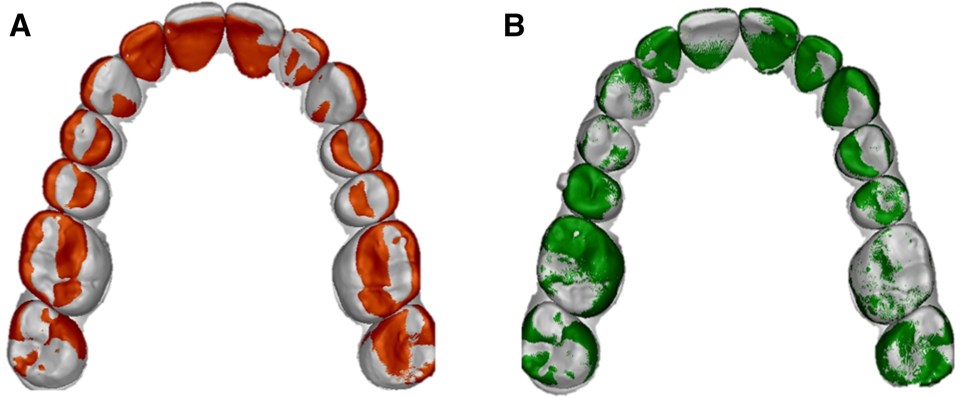
To obtain data on the accuracy of achieving the predicted outcome using Invisalign, we used the eModel compare software (version 9.0; GeoDigm Corporation, Falcon Heights, Minn). This particular software has been tested for reproducibility by Grauer et al and used extensively in previous studies comparing virtual treatment outcomes with achieved treatment outcomes. , The software uses a best-fit, 3-dimension superimposition algorithm that allows for the calculation of differences in both linear and angular dimensions for individual tooth positions between 2 digital models. The final stage of the initial set of aligners of each patient’s virtual treatment plan was exported from the ClinCheck (Align Technology Inc, Santa Clara, CA) software. If refinements were carried out, the initial scan from the refinement set was used as the actual achieved tooth movement. If no refinements were needed, a posttreatment intraoral scan was used. The models were then segmented and prepared using the eModel compare software. The dental arches were initially aligned globally, with the mesial-buccal cusps of the first molars and the contact point between the central incisors in each arch used as points for initial registration as described by Larson et al. This initial model registration was then refined with 30 automatic iterations using the closest-point algorithm. The individual teeth from the segmented (predicted tooth movement) model were then superimposed (and the discrepancies measured) on the analogous teeth of the unsegmented (achieved tooth movement) model. The software was set to attempt 30 iterations of the best-fit surface-based registration until the best-fit tooth surfaces were obtained ( Fig ).
The differences between achieved and predicted tooth positions were computed in linear (mesial-distal, buccal-lingual, and occlusal-gingival) and angular (tip, torque, and rotation) dimensions. Data from the patient’s dentition were organized into 4 categories: maxillary and mandibular anterior and posterior dentitions, with third molars excluded if present. The calculated differences between predicted and achieved tooth positions included positive and negative values based on the direction of the discrepancy; therefore, all values were converted into absolute values before data analysis. Because of the software’s ability to measure differences that are too small to be clinically relevant, the thresholds for clinically significant discrepancies were set at 0.5 mm for linear and 2° for angular measurements as per Grünheid et al, which is based on the American Board of Orthodontics model grading system. Intrarater reliability testing by intraclass coefficient correlation was performed by repeating the process of model preparation, segmentation, and measurement on 10 randomly selected patients for each of the 6 types of tooth movements. The measurements were performed at 3 time points at 2-week intervals.
Statistical analysis
The data were compiled using Excel (Microsoft, Redmond, Wash), and after that, statistical analyses were performed using SPSS statistical software (version 25; SPSS, Chicago, Ill). P values of less than 0.05 were considered statistically significant. Interval data were tested for normal intragroup distribution using the Shapiro-Wilk test; intergroup data distributions were tested using the Levene test. Independent t tests were used for normally distributed data, and Mann-Whitney U-tests were used if the data were not normally distributed. Chi-square tests were used for nominal data testing.
Results
The 2 groups were observed for pretreatment differences in sample size, age, gender, Angle classification, maxillary and mandibular irregularity index, and the number of initial aligners. Homogeneity was demonstrated with no significant differences using 2-tailed independent t tests for interval data and chi-square tests for ordinal data ( Table I ). Intraclass correlation coefficient tests demonstrated high intrarater agreement for all measurements using the eModel compare software ( Table II ).
| Groups | n | Age (y) | Gender (men:women) | Angle Class (I:II:III) | Mn irregularity index (mm) | Mx irregularity index (mm) | No. of initial aligners |
|---|---|---|---|---|---|---|---|
| DM | 45 | 30.1 ± 13.7 | 14:31 | 31:10:4 | 4.4 ± 2.6 | 5.2 ± 2.7 | 23.1 ± 10.2 |
| Control | 45 | 31.0 ± 11.5 | 11:34 | 31:9:5 | 5.3 ± 3.0 | 5.3 ± 2.6 | 23.2 ± 10.1 |
| P | 1.0 | 0.67 | 0.48 | 0.88 | 0.15 | 0.89 | 0.92 |
| Type of tooth movement | ICC | 95% Confidence intervals | |
|---|---|---|---|
| Lower bounds | Upper bounds | ||
| MD | 0.951 | 0.939 | 0.961 |
| BL | 0.996 | 0.996 | 0.997 |
| OG | 0.982 | 0.978 | 0.986 |
| Tip | 0.921 | 0.903 | 0.936 |
| Torque | 0.985 | 0.982 | 0.988 |
| Rotation | 0.966 | 0.959 | 0.973 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


