This case report describes the treatment of a boy, aged 13.6 years, whose ankylosed maxillary left central incisor had been avulsed and replanted 2.5 years earlier. Ankylosis of the tooth and adjacent alveolar process led to the development of infraocclusion, migration of adjacent teeth, midline deviation, and a vertical alveolar bone defect. Initially, distal tooth movement in the maxillary arch was performed with microimplant anchorage to gain space for repositioning the ankylosed tooth. Then a single-tooth osteotomy was performed in 1 surgical stage to allow for inferior repositioning of the tooth and bone. The ankylosed tooth was successfully leveled in the maxillary arch with a harmonic gingival margin. The total treatment period was 18 months, and the results were acceptable at 14 months after debonding.
Avulsion is a serious injury that causes damage to the periodontal ligament, alveolar bone, gingiva, pulp, and cementum. Replantation of avulsed teeth is frequently complicated by dentoalveolar ankylosis. This condition can result in replacement root resorption, in which the root is substituted by bone.
Tooth ankylosis is a localized fusion of cementum and surrounding alveolar bone with obliteration of the periodontal ligament and is apparently caused by mechanical, thermal, or metabolic trauma to the periodontal membrane during or after tooth eruption. Permanent incisors frequently become ankylosed, when the periodontal ligament is traumatically damaged, such as in the case of replantation after avulsion with a prolonged replantation time.
The diagnosis of ankylosis can be made by both clinical and radiologic evaluations. Clinical diagnosis can be made by infraocclusion, percussion, and mobility testing. However, the most important indicator of ankylosis is the lack of tooth movement with application of an orthodontic force. Total ankylosis is demonstrated radiographically by the absence of any periodontal membrane. However, it is difficult to identify when fusion occurs only in a small area or on the buccal or lingual surface. Radiographic examination has limited value in the early detection of ankylosis, because of the 2-dimensional image. Recent advancements have made it possible to measure the radicular volume involved in ankylosis, and its exact location on the tooth can be demonstrated by using computed tomographic imaging. This imaging technique with tridimensional reconstruction provides a positive diagnosis of ankylosis.
Treatment methods for ankylosed teeth include extraction, decoronation, restoration, surgical subluxation, ostectomy, osteocorticotomy, and distraction osteogenesis. Osteocorticotomy is a surgical procedure in which the intact ankylosed tooth and adjacent bone are either repositioned in 1 step or moved orthodontically. This technique does not correct the ankylosis, but it does permit optimal repositioning of the tooth.
In this case report, we present the treatment of a severely ankylosed maxillary central incisor that was brought into the arch by an individual osteotomy and by using an interdental space created by microimplant anchorage.
Diagnosis
The patient was a boy, aged 13.6 years, seeking esthetic orthodontic treatment for a severely ankylosed maxillary left central incisor, displaced 7 mm apically relative to the adjacent central incisor. A traumatic injury at the age of 11.5 years had resulted in the avulsion of the maxillary left central incisor, which was later replanted and followed by endodontic treatment. As the patient grew, the infraoccluded state of the maxillary left central incisor worsened, with discoloration from accompanying root resorption ( Fig 1 ).
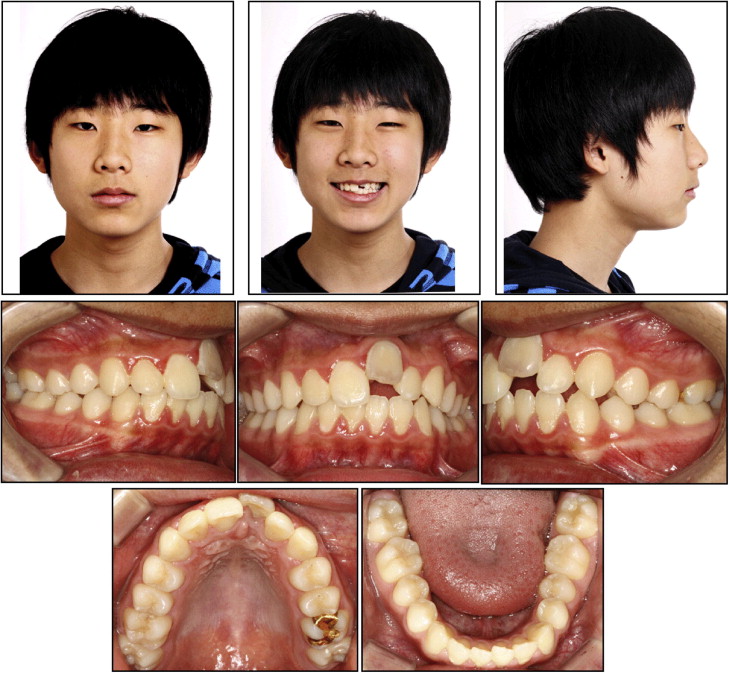
The patient had a well-balanced and symmetrical face, but a slightly convex soft-tissue profile. He also had an asymmetric smile line because of the ankylosed maxillary left central incisor and a poor appearance of the gray malpositioned tooth upon smiling ( Fig 1 ).
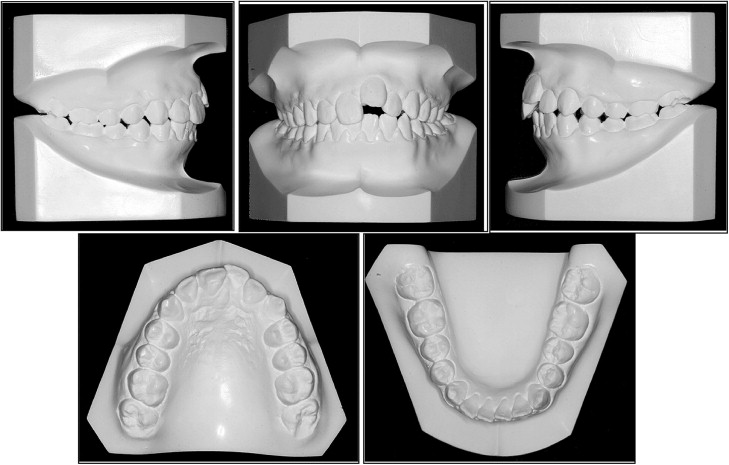
Intraorally, he had Class II canine relationships, particularly on the left side. The maxillary left central incisor was infraoccluded and in a labial position; the gingival level of this tooth was 7 mm higher than that of the adjacent teeth. The left anterior occlusion showed an open bite, because the maxillary left central incisor was severely intruded ( Figs 1 and 2 ).
The lateral cephalometric analysis showed a mild skeletal Class II anteroposterior discrepancy with an ANB angle of 5.3° (SNA, 78.2°; SNB, 72.9°), and the vertical skeletal pattern was deemed normodivergent as evidenced by the Frankfort mandibular plane angle of 27.4°. The angle between Frankfort horizontal and the maxillary incisor axis of 126.2° indicated the labioversion of the maxillary ankylosed left central tooth, and the incisor mandibular plane angle of 98.5° reflected the proclination of the mandibular incisors ( Table ). The soft-tissue analysis showed mild lip fullness. The posteroanterior cephalogram showed a symmetrical facial contour. Dental asymmetry, in which the maxillary dental midline was shifted to the left of the facial midline, was present and had been caused by the ankylosed maxillary left central incisor causing tipping the adjacent teeth ( Fig 3 ).
| Pretreatment | Posttreatment | 14 months posttreatment |
|
|---|---|---|---|
| FMIA (°) | 54.1 | 53.1 | 52.1 |
| FMA (°) | 27.4 | 27.2 | 26.7 |
| IMPA (°) | 98.5 | 99.7 | 101.2 |
| SNA (°) | 78.2 | 77.3 | 77.6 |
| SNB (°) | 72.9 | 72.6 | 72.9 |
| ANB (°) | 5.3 | 4.7 | 4.7 |
| AO-BO (mm) | 4.6 | 3.5 | 3.4 |
| Occlusal plane angle (°) | 7.6 | 7.8 | 7.5 |
| FH to U1 (°) | 115.7 | 109.1 | 110.0 |
| FH to ankylosed U1 (°) | 126.2 | 107.9 | 108.5 |
| Z angle (°) | 65.7 | 69.2 | 70.0 |
| FHI (PFH/AFH) (%) | 67.0 (51.2/76.7) | 67.0 (52.0/78.2) | 69.0 (54.7/79.6) |
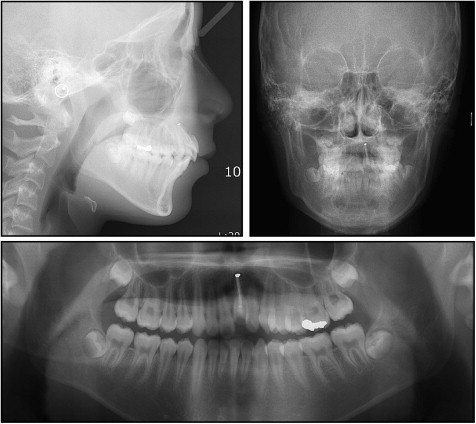
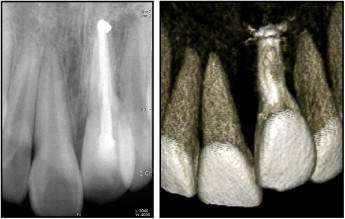
The panoramic radiograph showed a full complement of teeth, including developing third molars, and infraposition of the maxillary left central incisor. The alveolar process in this region had a severe deficiency in vertical development ( Fig 3 ). The periapical radiograph and 3-dimensional computed tomography image showed ongoing replacement resorption of the ankylosed maxillary left central incisor, which had been endodontically treated ( Fig 4 ). There were no significant signs or symptoms of temporomandibular disorders.
Treatment objectives
The treatment objectives were to (1) correct the Class II occlusion, (2) correct the axes of the tilted teeth, (3) correct the midline, (4) obtain a normal incisor relationship, (5) improve the smile, and (6) correct the osseous and gingival margins in the ankylosed region (maxillary left central incisor).
Treatment objectives
The treatment objectives were to (1) correct the Class II occlusion, (2) correct the axes of the tilted teeth, (3) correct the midline, (4) obtain a normal incisor relationship, (5) improve the smile, and (6) correct the osseous and gingival margins in the ankylosed region (maxillary left central incisor).
Treatment alternatives
Several treatment alternatives were explored in regard to the ankylosed tooth.
- 1.
Extract the ankylosed tooth and close the space orthodontically.
- 2.
Perform an osteotomy distraction osteogenesis and immediately reposition the dentoalveolar structures.
- 3.
Perform an osteotomy of the segment with immediate repositioning of the dentoalveolar structures.
The third treatment plan was chosen for this patient, considering several major factors: the ankylosed tooth, the replacement resorption of root, and the moderate bone defects.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


