During orthodontic treatment with miniscrews, complications such as aphthous ulceration, soft-tissue coverage of the miniscrew head, soft-tissue inflammation, infection, and peri-implantitis can occur. Good hygiene can prevent inflammation by infection but does not prevent traumatic oral mucosal lesions at the buccal mucosa. The purpose of this article was to describe the use of a physical barrier—a light-cured temporary filling material—to cover the miniscrew head and prevent soft-tissue trauma.
Osseous anchorage with dental implants was introduced in the 1980s; moreover, it was in 1997 that Kanomi introduced miniscrews, a variation of surgical fixation screws. Miniscrews can be placed in various alveolar bone locations, and numerous applications have been presented in literature. Nevertheless, complications can arise during miniscrew placement, such as trauma to the periodontal ligament, dental root, or nerves, nasal and maxillary sinus perforation, and subcutaneous air emphysema. Complications during orthodontic loading such as aphthous ulceration, soft-tissue coverage of the miniscrew head, soft-tissue inflammation, infection, and peri-implantitis can also occur. Traumatic lesions to soft tissues do not appear to be a direct risk factor for miniscrew stability, but their presence might predict greater soft-tissue inflammation. The placement of a healing abutment, a wax pellet, or a large elastic separator over the miniscrew head, with daily use of chlorhexidine (0.12%, 10 mL), typically prevents ulceration and improves patient comfort. Covering the miniscrew head to prevent soft-tissue damage is not a current procedure in orthodontics; therefore, the aim of this article was to present the alternative use of a dental material for this purpose.
Case report
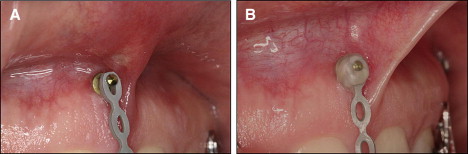
After miniscrew placement, the soft tissues can be damaged by friction. The patient in Figure 1 had a mini-implant placed between the central incisors. Within 48 hours, an ulceration appeared in the frenulum ( Fig 1 , A ), despite an elastic chain on the miniscrew head. Resin was placed over the miniscrew head, and, after 4 days, the tissue was healthy ( Fig 1 , B ).
An alternative covering material and application technique—a light-cured temporary filling material, Bioplic (Biodinâmica, Ibiporã, Paraná, Brazil)—has been used for years in the orthodontic department at the Federal University of Rio de Janeiro in Brazil to cover miniscrew heads and prevent patient discomfort. This material has a viscous and elastic consistency after polymerization, allowing easy placement and removal. Some clinicians use composite resin to cover the miniscrew head, but burs are required to remove the resin.
The placement technique is simple and fast. Relative isolation is required, and it is necessary to dry the miniscrew head. Use a tooth sculpture tool (or a similar instrument), to shape the filling material and then light-cure it for 40 seconds ( Fig 2 ). The material is easily removed with a probe ( Fig 3 ).



