Developmental absence of maxillary lateral incisors is not uncommon in orthodontic patients. Treatment depends on a number of factors, including skeletal pattern, type of malocclusion, overjet, and the shape and color of the canines. Management can be broadly divided into space closure, space opening or redistribution, and prosthetic replacement. The purpose of this article was to report the treatment of a girl with an Angle Class I malocclusion with missing maxillary lateral incisors and severe crowding in the mandibular labial segment. Treatment included preadjusted fixed appliances, extraction of the mandibular first premolars, and space closure of the maxillary labial segment space with the canines substituted for the maxillary lateral incisors.
Hypodontia is the developmental absence of at least 1 tooth. The incidence of missing maxillary lateral incisors is 1% to 2% in white populations. The etiology of hypodontia can be genetically determined and arises as a familial condition. The condition is more common bilaterally than unilaterally and can be associated with impacted maxillary canines. This condition causes several problems, including unsightly spacing between the anterior teeth, and drifting and rotation of the central incisors and the canines. In unilateral cases, these effects are asymmetric and can result in a midline shift. Furthermore, dental health problems might arise because of food impaction as a result of tipped teeth. A suspected absence of the maxillary permanent lateral incisor should be confirmed radiographically if the tooth has failed to erupt by the age of 9 years, or within 6 months of the contralateral tooth.
The management of missing maxillary lateral incisors often needs a multidisciplinary approach and can be broadly divided into space closure, space opening, and space redistribution. A number of factors should be considered in the management of such patients. These include patient factors: age, medical history, motivation, and attitude toward orthodontic treatment. Other factors include skeletal pattern, type of malocclusion, number of missing teeth, size, shape, and the gingival margin of the maxillary canines. In this case report, an adolescent girl complained of the appearance of her maxillary anterior teeth because of developmentally absent lateral incisors and crowding in the mandibular arch.
Diagnosis and etiology
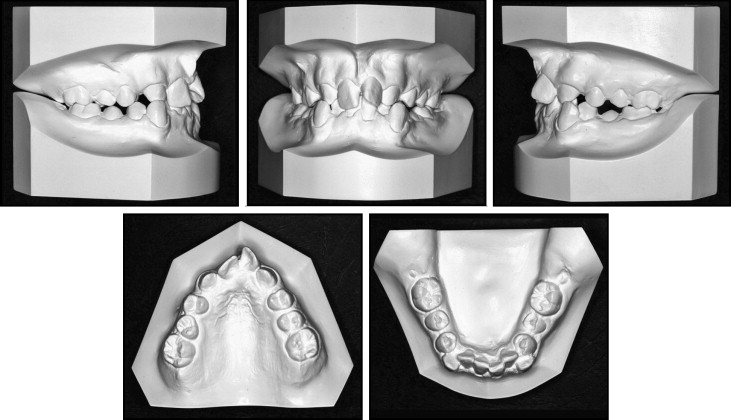
This girl, aged 14.6 years, had an Angle Class І malocclusion on a mild Class ІІ skeletal pattern with reduced Frankfort mandibular plane angle and lower anterior face height. There was no facial asymmetry, and the lips were competent with a low smile line ( Fig 1 ). In the intraoral assessment, her oral hygiene was fair but needed improvement before orthodontic treatment. The erupted teeth were as follows.
| 6 5 4 3 1 | 1 3 4 5 6 |
| 7 6 5 4 3 2 1 | 1 2 3 4 5 6 7 |

Both maxillary and mandibular left first molars were hypoplastic but not carious. Fissure sealants were present occlusally in all first molars. From the history and clinical examination, these teeth did not cause any problem to the patient (eg, sensitivity), and the long-term prognosis was good. The maxillary arch had spacing, whereas the mandibular arch was severely crowded. Overjet was 5.5 mm, and overbite was deep with palatal impingement. The molar relationship was Class I on both sides, and the incisor relationship was Class II Division 2 ( Fig 2 ). The maxillary canines were in crossbite. Furthermore, the maxillary left central incisor and the maxillary right second premolar were rotated; these might cause some concern in terms of stability and risk of relapse. The mandibular left second premolar was partially erupted. In addition, space analysis showed that the space requirement in the mandibular arch was 14 mm.
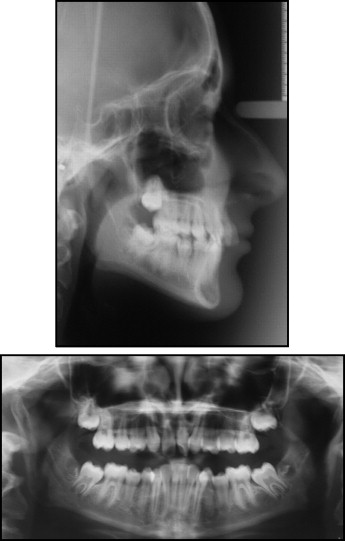
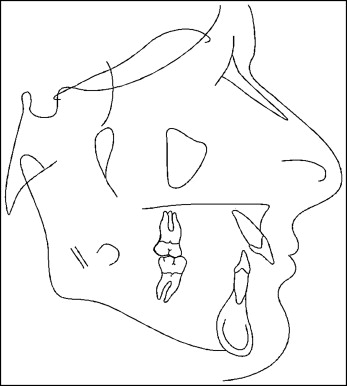
The dental panoramic tomogram confirmed the presence of all permanent teeth except the maxillary lateral incisors and the third molars. Teeth yet to erupt were the maxillary and mandibular second molars and the mandibular third molars ( Fig 3 ). Root length and morphology appeared normal. In the cephalometric assessment ( Fig 4 and Table ). The ANB value was 3°, which suggested a Class І skeletal pattern. However, by applying the Eastman correction (SN/Max 10°), the corrected ANB was 5°, which indicated a mild Class ІІ skeletal pattern. The mandibular incisor inclination was retroclined at 80°. The maxillary left central incisor was proclined at 118°, and the maxillary right central incisor appeared retroclined. The lower anterior face height was reduced, and the mandibular incisor to the APo line was within normal limits. The lower lip was positioned posteriorly to the E-line.
| Variable | Pretreatment | Normal ∗ | Predebond | Overall change |
|---|---|---|---|---|
| SNA | 86° | 82° ± 3° | 85° | −1° |
| SNB | 83° | 79° ± 3° | 82° | −1° |
| ANB | 3° | 3° ± 1° | 3° | 0 |
| Maxillary incisor to maxillary plane angle | 118° | 108° ± 5° | 113° | −5° |
| Mandibular incisor to mandibular plane angle | 80° | 92° ± 5° | 90° | −10° |
| Interincisal angle | 142° | 133° ± 10° | 130° | −12° |
| Maxillary-mandibular planes angle | 20° | 27° ± 5° | 23° | 3° |
| Face height ratio | 52% | 55% | 54% | 2% |
| Mandibular incisor to APo line | −2 mm | 0–2 mm | 1 mm | 3 mm |
| Lower lip to Ricketts’ E-plane | −4 mm | −2 mm | −1 mm | 3 mm |
∗ Normal values for white subjects taken from Houston et al.
The malocclusion was complicated by the developmentally absent maxillary lateral incisors, increased and complete overbite, severe crowding in the mandibular arch and the crossbite involving the maxillary canines. The genetically inherited skeletal pattern and the reduced vertical proportions contributed to the malocclusion. In addition, the high lower lip line contributed to the retroclination of the maxillary right central incisor.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


