An orthodontic miniplate tube device, the C-tube, was designed for use in patients for whom a conventional miniscrew is not suitable, such as those with narrow interradicular spaces, extended maxillary sinuses, dilacerated roots, or severe alveolar bone loss. After local anesthesia, 2 parallel horizontal incisions are made in the area of placement, and the periosteum is elevated. The C-tube is slipped under the mucosal flap and fixed with self-drilling miniscrews (diameter, 1.5 mm; length, 4 mm). Because the screws are short, there is adequate retention in the alveolar plate, and the clinician can avoid the increased morbidity of anchoring to the zygomatic buttress. This makes placement possible with superficial anesthesia. A small rolled tube at the head part can act as an orthodontic tube and accommodate archwires or as a hook to attach orthodontic elastics. However, in some patients with pneumatization or systemic diseases, such as diabetes mellitus, or in heavy smokers, cross-type C-tubes with longer miniscrews are recommend for better stability. This new type of orthodontic miniplate can be an effective alternative to conventional 1-component screws or miniplates in complex situations.
Recently, a number of case reports with skeletal anchorage as orthodontic anchorage have been presented. Several types of skeletal anchorage devices, including miniscrews, onplants, and miniplates, have been introduced, and the most popular is the miniscrew. Miniscrews are reasonably cost low, easy to place and remove, and small, and can be implanted in many locations in the oral cavity. These strong points might be the reasons for their popularity. But their placement is usually between the dental roots; this renders them an obstacle to many desired tooth movements. To overcome this weak point, clinical trials to place miniscrews apart from the dental apparatus—eg, the palatal area—have been performed. But this location complicates the biomechanical design and is usually limited to the maxilla.
There have been previous reports about surgical miniplates as orthodontic anchorage. These miniplates do not interfere with tooth movement and can withstand heavier and more dynamic forces than miniscrews because of multi-screw retention. However, the surgical miniplate is not ideal for orthodontic purposes because its shape is not designed for orthodontic use, and placement is not easy.
Still, miniplates are useful when the anatomic situation prevents the use of a miniscrew. Several designs are suitable for orthodontic purposes. Sugawara et al developed a new design of miniplate anchored to the zygomatic buttress and named it the “skeletal anchorage system.” De Clerck and Cornelis showed patients treated with miniplates and various additive components. But these systems still require relatively longer retentive screws and are placed in deeper anatomic sites, requiring invasive surgery. Simpler designs might encourage orthodontists to place the device.
The C-tube was developed exclusively for orthodontic purposes with the concept of simple design and small size for easy placement. Clinical experiences have proved that this system can work as a good auxilliary orthodontic appliance and also as an appliance to partly replace orthodontic brackets. The purposes of this article were to introduce the C-tube primarily when miniscrews are not applicable and to show the various principles of clinical applications.
C-tube and orthodontic mechanics
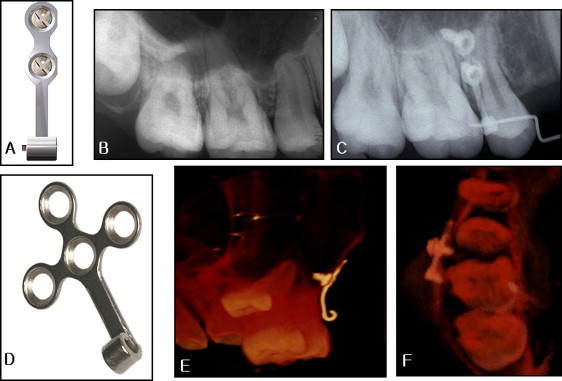
C-tubes are titanium miniplates with a 0.036-in diameter hole in the tube. They have 2 to 4 holes (diameter, 1.5 mm) and lengths of 4 to 7 mm; they are self-drilling miniscrews (KLS Martin, Tuttlingen, Germany, Jin Biomed Co., Bucheon, Korea) ( Fig 1 ).
The C-tube is anchored to the cortical bone near the posterior teeth, instead of the zygomatic buttress. C-tube placement requires a minimum of dissection compared with the buttress site.
Two types of C-tube have developed: I and cross. The I-type C-tube is fixed with 2 drill-free miniscrews and applied in the posterior maxillary area if there are narrow interradicular spaces or dilacerated roots, or in the anterior maxilla with a prominent labial frenum ( Fig 1 , A-C ). Cross-type C-tubes are used when there is severe pneumatization of the maxillary sinus or when distalization of the dentition is planned. The cross-type C-tube is fixed with 2 to 4 drill-free 4-mm miniscrews according to the quality of bone and the direction of the orthodontic force vector. Although a 4-mm miniscrew might seem short, the use of several screws gives good stability to the miniplate even in thin cortical bone. Also, these miniscrews are short enough not to touch dental roots and not to interfere with tooth movement. The C-tube can be placed in various region of the oral cavity and is valuable where absolute anchorage is needed ( Fig 2 ).
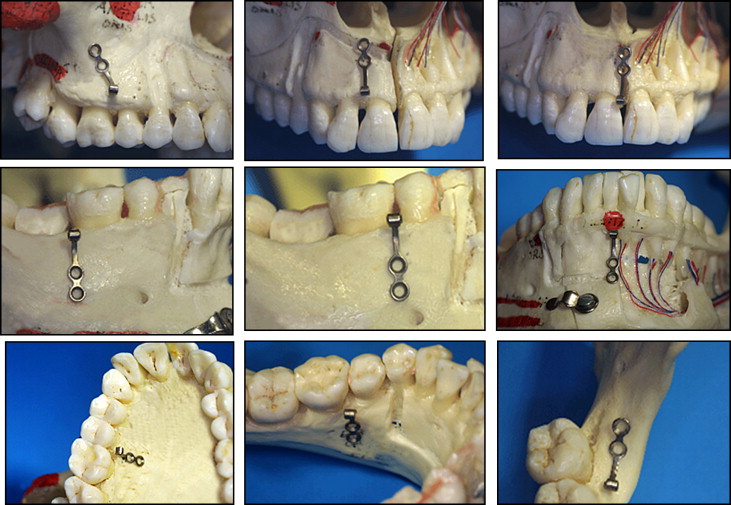
A C-tube in the posterior maxillary area can be used for intrusion and distalization of posterior teeth ( Fig 2 , A ) and also for intrusion of anterior teeth ( Fig 2 , B and C ). In the maxillary area of the mental foramen, it can be used for intrusion or distalization of the mandibular posterior teeth and intrusion of anterior teeth ( Fig 2 , D-F ). Also, it is applicable for lingual orthodontics and can be placed on the retromolar pad with the rolled tube exposed in the oral cavity ( Fig 2 , G-I ).
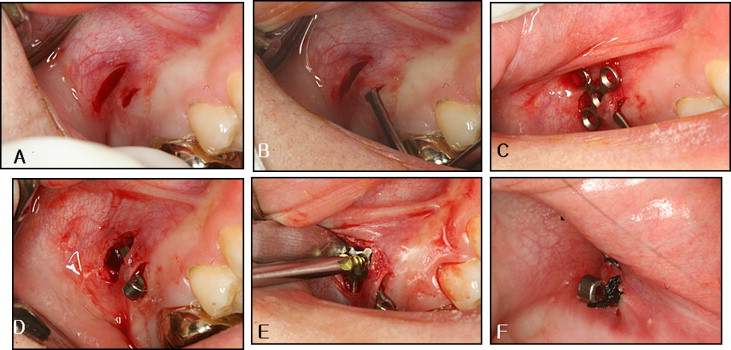
Usually, the C-tube is placed in alveolar bone between the dental roots or in cortical bone above the alveolar bone ( Fig 3 ). These areas are much lower and more accessible than the zygomatic buttress where a conventional miniplate is usually placed. The intraoral exposure part of the C-tube is placed at the border between attached and movable mucosa. The head part of the C-tube should be adjusted with care so that it will not be covered by the mucosa.
- 1.
Inject local anesthesia and wait for 10 minutes for complete diffusion of the anesthesia.
- 2.
Make a horizontal incision with a number-15 blade where the head of C-tube is to be exposed and then make another 3-mm long horizontal incision 2 mm apical and parallel to the first one ( Fig 3 , A ).
- 3.
Lift the periosteum carefully with a periosteal elevator ( Fig 3 , B ).
- 4.
Conform the C-tube to the exposed bony surface with a bending pliers.
- 5.
Place the C-tube on the bone surface through the second horizontal incision ( Fig 3 , C ), expose the tube part to the oral cavity, and then fix the C-tube with self-drilling miniscrews (diameter, 1.5 mm; length, 4 mm) placed through the second horizontal incision ( Fig 3 , D and E ).
- 6.
Suture the incised area with 4-0 silk ( Fig 3 , F ).
- 7.
Prescribe nonsteroidal anti-inflammatory drugs and antibiotics for 3 days. Remove the suture material 1 week later.
The removal procedure includes the following steps.
- 1.
After local anesthesia, make a vertical incision on the miniscrew area with a number 15 blade.
- 2.
Unscrew the miniscrews and remove the C-tube through the incision. Sometimes it is necessary to increase the opening for the head part to slip through the tissue.
- 3.
Suture the incision area with 4-0 silk.
- 4.
Prescribe nonsteroidal anti-inflammatory drugs and antibiotics for 3 days. Remove the suture material 1 week later.
Clinical applications of the C-tube
The C-tube can be used for en-masse retraction without posterior appliances. The C-tube is applied on the maxillary anterior teeth without attached appliances to the posterior dentition in maximum anchorage cases. It can replace brackets on the posterior dentition through accommodation of the posterior part of the archwire into its tube without losing control of the anterior teeth. It resists heavy and dynamic loads because of several miniscrews. Also, various elastics, power chains, and archwires can be easily applied to the 0.9-mm diameter hole in the tube.
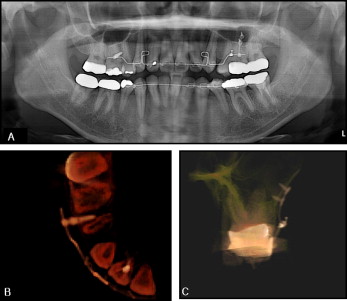
A 30-year-old woman visited our orthodontic clinic complaining of lip protrusion. After a complete analysis, she was diagnosed as having Class II bidentoalveolar protrusion; the treatment plan included extraction of the 4 first premolars and temporary skeletal anchorage devices TSADs to enable en-masse retraction ( Figs 4 and 5 ). A sand-blasted with large grit and acid-etched surface-treated mini-implant (C-implant, Cimplant Co., Seoul, Korea) was implanted between the maxillary right second premolar and first molar, but, on the left side, a narrow interradicular space and extended maxillary sinus contraindicated the use of the C-implant ( Fig 4 , A and B ). Instead, an I-type C-tube was placed with 2 self-drilling miniscrews ( Fig 4 , C ). The miniscrew and the C-tube eliminated any need for bracketed appliances on the maxillary posterior dentition. The archwire passed through the head of the C-tube. After 19 months, resolution of anterior protrusion and closure of extraction space were achieved ( Fig 5 ).

The C-tube can be used in the same way with lingual appliances ( Fig 6 ).
C-tubes can be used for vertical correction. I-type C-tubes can be used for intrusion of the maxillary incisors ( Fig 7 ). A 34-year-old woman with a deep anterior overbite and a lingually blocked maxillary left lateral incisor was treated with an I-type C-tube ( Fig 7 , A and B ). Her blocked lateral incisor was extracted, and the C-tube was placed between the maxillary right central and lateral incisors. Intrusion force was applied with elastic chain between the C-tube and the archwire. Intrusion took 4 months; this allowed bracket to be placed on the mandibular anterior teeth ( Fig 7 , C and D ). The total treatment period was 15 months.
Another patient required intrusion of the mandibular anterior teeth. A 32-year old man was diagnosed with a Class II anterior deepbite malocclusion with anterior spacing. We placed 2 miniscrews on the maxillary teeth and an I-type C-tube on the mandibular anterior teeth ( Figs 8 and 9 ). The maxillary miniscrews (C-implants: diameter, 1.8 mm; length, 8.5 mm) were used for anterior retraction, and a C-tube on the mandibular anterior teeth was used for intrusion. The C-tube was fixed to cortical bone under the mucosa, avoiding the roots of the incisors, and the head of the C-tube was exposed through the attached gingiva. This minimized inflammation. Four millimeters of intrusion occurred after 3 months of active intrusion ( Fig 9 ).


