and Angela J. Yoon1
(1)
Columbia University College of Dental Medicine and Department of Pathology and Cell Biology, Columbia University Medical Center, New York, NY, USA
It is not uncommon to encounter ulcers in pediatric patients. The vast majority of these ulcerations are transient and of traumatic or viral origin. Canker sores are also common in pediatric patients. The presence of persistent or continually recurring ulcers can be indications of an underlying medical condition or systemic disease (See Part 2). Vesiculo-bullous diseases such as mucosal pemphigoid and pemphigus vulgaris might appear on the differential diagnoses for multiple chronic ulcers in an adult patient, but these entities are rare in children and adolescents and therefore will not be covered.
|
Oral ulcerations
|
|---|
|
Viral ulcers
|
|
Primary herpetic gingivostomatitis
|
|
Recurrent herpetic infection
|
|
Herpangina
|
|
Hand-foot-and-mouth disease
|
|
Non-viral ulcers
|
|
Traumatic ulcer
|
|
Canker sores
|
|
Erythema multiforme
|
|
Impetigo
|
3.1 Acute Herpetic Gingivostomatitis (Primary Herpes)
Acute herpetic gingivostomatitis is the symptomatic presentation of the initial exposure to the herpes simplex virus 1 (HSV-1). HSV-1 is ubiquitous and most individuals are exposed to the virus by age five. The initial infection in the majority of patients is subclinical; however, up to 30 % of children develop acute gingivostomatitis. It develops approximately 1 week after initial contact with an infected, often asymptomatic child or adult.
Clinical Appearance
Oral lesions consist of numerous tiny vesicles, which rupture rapidly to form painful irregular ulcerations covered by yellow–gray membranes. Submandibular lymphadenitis, halitosis, and refusal to eat and/or drink are often accompanying findings. The lesions typically appear after about 3–4 days of prodromal symptoms, i.e., fever (>38 °C (100.4 °F)), anorexia, irritability, malaise, sleeplessness, headache.
Etiology
Herpes simplex virus 1 (HSV-1).
Location
The lesions involve both keratinized and nonkeratinized mucosa. The gingiva is almost always involved – often appearing inflamed and painful.
Differential Diagnosis
Erythema multiforme and aphthous stomatitis.
Treatment
Mild lesions typically heal without scarring in about a week, but healing can take up to 14–21 days in severe cases. Treatment consists of palliative care – including maintaining fluid intake and good oral hygiene. Refusal to drink can result in dehydration, which is the most frequent complication. Topical anesthetics (i.e., viscous lidocaine) and a mouth rinse containing Benadryl and Kaopectate can be prescribed as a rinse-and-spit or can be applied to the lesions using cotton swabs. OTC children’s Tylenol can also be helpful.
If the child is immunocompromised or if the child is less than 6 months of age, the patient’s pediatrician should be notified.
Important Reminder
Parents should be cautioned to ensure child stays hydrated and maintains nutrition. Parents must be diligent to ensure infants and young children keep their hands out of their mouths as the virus can spread to the skin and eyes. Untreated herpetic infections of the eye can result in blindness.
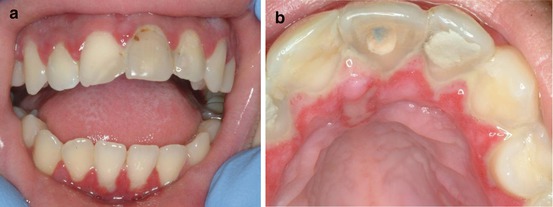
Fig. 3.1
(a, b) Primary herpetic gingivostomatitis. Fourteen year old presented with a 3 day duration of painful inflamed gingiva and coalescing irregular ulcerations of the attached gingiva and anterior hard palate. Patient also had a sore throat and low grade fever. Lesions resolved by the following week with only palliative care

Fig. 3.2
Primary herpetic gingivostomatitis. Five year old with painful, enlarged, and erythematous gingiva
Clinical Question
Should an antiviral medication be prescribed for a patient with primary herpetic gingivostomatitis?
Answer: Antiviral medications are most effective when taken at the onset of symptoms. Typically, when a patient with primary herpes presents to the dentist he or she has already had the lesions for a few days. Therefore, antiviral medications are typically not prescribed. Exceptions would be if the patient is very young or immunocompromised and in those cases it is best to consult with the patient’s pediatrician.
3.2 Herpes Labialis and Recurrent Intraoral Herpes
Reactivation of the herpes simplex virus 1 (HSV-1) in a previously exposed child can result in intraoral or extraoral lesions. The most common clinical form of recurrence herpes is herpes labialis, commonly known as a “cold sore” Intraoral recurrent herpes involves keratinized tissue, often the hard palate. Both can cause discomfort. Herpes labialis is often preceded by a tingling or itching (prodromal signs) sensation at the site before the lesions develop involving the skin of lips.
Clinical Appearance
Lesions consist of numerous tiny vesicles, which rupture rapidly to form small ulcers. Intraoral lesions are covered by yellow–gray membranes, whereas cutaneous/labial ulcers appear crusted.
Etiology
Herpes simplex virus 1 (HSV-1).
Location
Herpes labialis occurs on skin of the lip; recurrent intraoral herpes involve the keratinized mucosa only (i.e., palate).
Differential Diagnosis
-
Herpes labialis: impetigo (see pg 31), traumatic ulcer
-
Intraoral recurrent herpes simplex: The localized involvement and restriction to keratinized mucosa can be used to exclude a number of entities including: erythema multiforme, aphthous stomatitis, primary herpetic gingivostomatitis, and varicella zoster.
Treatment
Mild lesions typically heal without scarring in about a week, but healing can take 14–21 days in severe cases. Prescription topical antiviral creams (i.e., Penciclovir 1 % cream (Denavir)) or OTC topical antiviral cream Docosanol cream 10 % (Abreva) can be helpful although they are most beneficial when applied at the earliest sign of an outbreak.
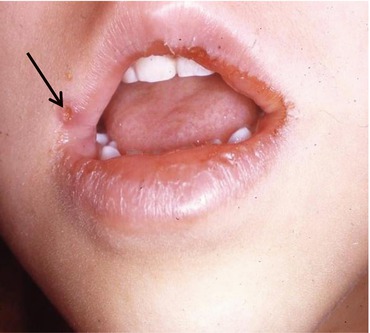
Fig. 3.3
Herpes labialis. Focal ulceration of the upper lip at the vermilion border

Fig. 3.4
Herpes labialis. Irregularly shaped and focally crusted ulceration of the upper lip
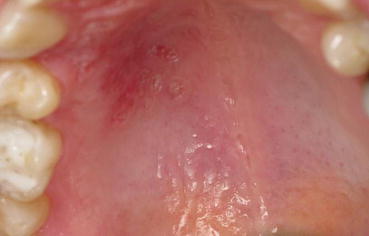
Fig. 3.5
Recurrent intraoral herpes. Multiple punctate ulcers which have begun to coalesce affecting the hard palate

Fig. 3.6
Recurrent intraoral herpes. Multiple punctate ulcers of the attached (keratinized) gingiva
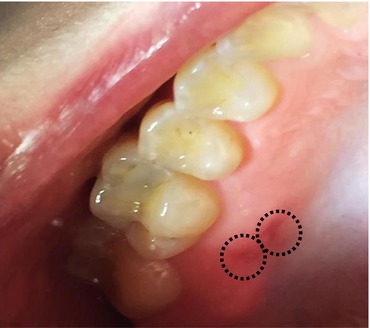
Fig. 3.7
Recurrent intraoral herpes. Two irregularly shaped superficial ulcers of the posterior hard palate. The lesions are the result of multiple punctate ulcers which had coalesced
Important Reminders
Although the fluid-filled vesicles are the most infectious stage, all stages can be contagious. Therefore, the dentist must decide whether or not to treat a child with an active infection. If he/she decides to treat the patient, the dentist must avoid spreading the virus to other areas of the child’s mouth and face.
Dental treatment can cause reactivation of the herpes virus, and it is not uncommon for herpes labialis or introaoral recurrent herpes to occur within 3 days of a dental procedure. The intraoral lesions typically occur on the palate or gingiva adjacent to the teeth which were worked on.
3.3 Herpangina
Herpangina is a highly contagious, symptomatic, self-limiting, viral infection. Patients present with a sudden high fever, sore throat, headache, neck pain, and loss of appetite. Oral lesions affecting the posterior oral cavity form within 2 days of onset of symptoms. Most cases occur in the summer and fall, affecting mostly infants and young children. It occasionally occurs in adolescents and adults. Typically spreads via the fecal-oral route or by respiratory droplets.
Clinical Appearance
A relatively few number (often <6) of 1–2 mm red macules or grayish plaques form on the soft palate or tonsillar pillars. The lesions form into vesicles and then ulcerate, resulting in shallow ulcers, 2–4 mm in size with surrounding erythema, resembling oral apthae.
Etiology
Most often Coxsackie virus A, can also be caused by Coxsackie virus B or Echoviruses.
Location
Most often soft palate and/or tonsillar pillars, can occur on the uvula, or tongue.
Differential Diagnosis
Aphthous stomatitis, strep throat, other viral infection (i.e., hand foot and mouth disease, varicella zoster, primary herpes, mononucleosis, etc.)
Treatment
Herpangina is self-limiting and lesions resolve in less than 7 days. Antiviral medications are not effective. Treatment consists of supportive care – including maintaining fluid intake. Eating popsicles can also help soothe a sore throat. Topical anesthetics (i.e., viscous lidocaine) and/or a mouth rinse containing Benadryl and Kaopectate can be prescribed as a rinse-and-spit or can be applied to the lesions using a couple of cotton swabs. OTC children’s Tylenol can also be helpful.
If the child is immunocompromised or if the child is less than 6 months the patient’s pediatrician should be notified.



Fig. 3.8
Herpangina. Several 1–2 mm red macules of the soft palate, which will form vesicles and ulcerate
Fig. 3.9
Herpangina. Small vesicles of the soft palate with peripheral erythema. The vesicles ulcerate to form shallow ulcers
Fig. 3.10
Herpangina. Shallow, aphthous-like ulcers of the uvula and soft palate



