Ocular hypertelorism is a congenital craniofacial malformation characterized by excessive distance between the eyes. It is one of the most expressive deformities of the human face. The aim of this case report was to discuss clinical aspects associated with the diagnosis, planning, and treatment of an orthodontic patient with ocular hypertelorism.
Ocular hypertelorism, a congenital craniofacial malformation characterized by excessive distance between the eyes, is one of the most expressive deformities of the human face. This condition affects children of normal intelligence, but the majority of times it is associated with other deformities (normally stemming from syndromes) involving the nose, cranium, and bones of the midface.
The etiologic factors responsible for hypertelorism remain unknown, but possible pathogenetic mechanisms include (1) early ossification of the lesser wings of the sphenoid; (2) failure of the nasal capsule development, allowing the primitive brain vesicle to protrude into the space normally occupied by the capsule; (3) abnormalities in the migration of the mesenchyma of the crest of the neural cells; and (4) altered blood flow in the region of the frontonasal process.
Although a number of studies on ocular hypertelorism have been published, most address genetic aspects and the surgical approach of treatment. Although the clinical manifestations of ocular hypertelorism have a significant effect on different structures of the craniofacial complex, no studies were found focusing on the orthodontic aspects of persons with this condition.
The aim of this study was to discuss the clinical aspects associated with the diagnosis, planning, and treatment of an orthodontic patient with ocular hypertelorism.
Diagnosis and etiology
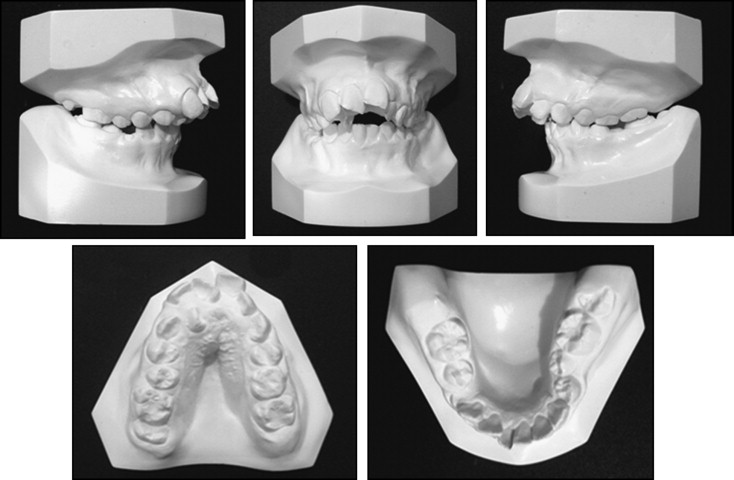
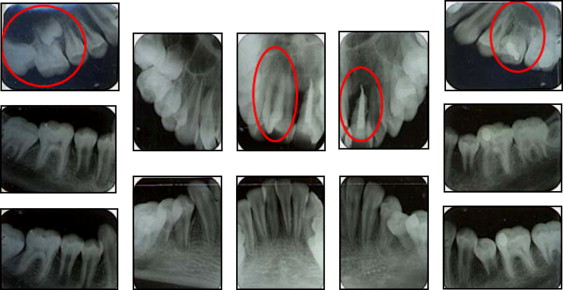
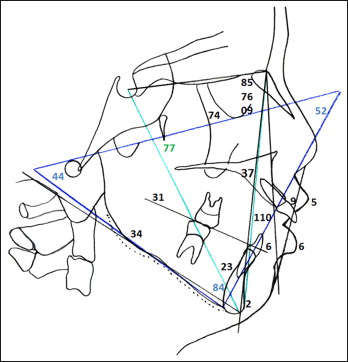
An 8-year-old girl sought treatment at the clinic of the Specialization Course in Orthodontics of the University of Itauna in Brazil. She exhibited facial asymmetry, ocular hypertelorism, increased lower third of the face, convex profile, acute nasolabial angle, hypotonia of the lower lip, and absence of lip seal. The oral examination showed that she was in the mixed dentition with an Angle Class II malocclusion. The overjet was 13 mm, and she had an anterior open bite and a bilateral posterior crossbite. The maxillary arch was atresic and crowded, and the mandibular arch had a diminished perimeter ( Figs 1 and 2 ). The radiographic examination showed the following: agenesis of the maxillary left second premolar; a supernumerary lateral incisor and a supernumerary premolar on the right side; history of trauma, endodontic treatment, and resorption of the maxillary left central incisor; and root resorption of the maxillary right first molar caused by the second molar ( Figs 3 and 4 ). The cephalometric evaluation showed that most dental and skeletal parameters were outside the standards of normality, and there was a tendency toward vertical growth ( Fig 5 ). The parents reported that the patient had undergone surgery at the Lucile Salter Packard Children’s Hospital in Stanford, California, for the correction of hypertelorism 2 years earlier.


Hypertelorism can be caused by numerous congenital defects in the development of the face and cranium or result from trauma. It might also be confused with many types of pseudohypertelorism, in which there is broadening of the interorbital distance because of an abnormality in the width of the bone between the sockets. True hypertelorism is associated with diverse congenital deformities, but there are 4 main groups: pure hypertelorism (Greig’s syndrome), characterized by broadening of the nose and eyes, short and swollen fingers, heavy eyelids, and lateral exotropia; hypertelorism associated with frontal encephalic hernia or excess skin along the midline; hypertelorism associated with severe lateral facial clefts and clefts of the lip and palate; and acrocephalosyndactyly hypertelorism (Apert’s syndrome), a syndrome of trisomy 21 and other defects that result from autosomal dominant genes. In the case described here, the patient had no neurologic impairment. She had intelligence proportional to girls of her age and exhibited concern and considerable interest about improving her facial appearance.
Treatment objectives
The treatment objectives were to extract the supernumerary teeth, eliminate the crowding in the maxillary and mandibular arches, correct the posterior crossbite, eliminate the anterior open bite, promote passive lip seal, and achieve a Class I skeletal and dental pattern. A further aim was to improve the esthetics of the nose through rhinoplasty.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


