This case report describes the treatment of an adult patient who had a Class II Division 1 malocclusion with a severe overjet (13.5 mm), a deep overbite (7 mm, 100%), and spacing between the maxillary anterior teeth. The purpose of this report is to demonstrate the importance of developing an individualized treatment plan, tailored to the patient’s specific dental and skeletal problems, as well as to his or her needs and desires. Although all indications pointed to a surgical intervention for this patient, her reluctance to undergo orthognathic surgery led to an alternative treatment, which yielded a satisfactory result.
Class II Division 1 malocclusions are characterized primarily by the mandibular canines and molars in distal relationships relative to the corresponding maxillary teeth, as well as by protrusion of the maxillary anterior teeth. Treatment planning for such patients must take into consideration numerous factors, including the soft-tissue profile, interlabial space, ratio of upper to lower face height, inclination of the occlusal plane, overbite, severity of the skeletal and dental Class II relationships, growth potential, and posttreatment stability.
When considering orthodontic treatment for adults with such malocclusions, additional factors must be taken into account. Treatment goals and outcomes might be affected by large restorations, missing teeth, periodontal status, loss of papillae, gingival recession, and bone loss. An interdisciplinary approach, including surgical intervention, is usually required. This case report illustrates a severe skeletal discrepancy in an adult that was successfully treated without orthognathic surgery.
Diagnosis and etiology
The patient was a white woman, 51 years of age at the time of consultation. Her chief complaint was the unesthetic appearance of her smile. She also mentioned frequent irritation of her cheeks and palate, as well as difficulty in chewing and maintaining proper oral hygiene, all of which she attributed to her malpositioned teeth. She had regular checkups with her general dentist and, in the past, had been treated by a periodontist. She indicated some hypersensitivity of the maxillary anterior teeth to cold. She also mentioned that she had occasional episodes of snoring, as well as some pain and clicking in the area of the right temporomandibular joint. Aside from an allergy to nuts, she was in good health and took no medication. The etiology of her malocclusion appeared to be hereditary; she stated that her father had a similar condition.
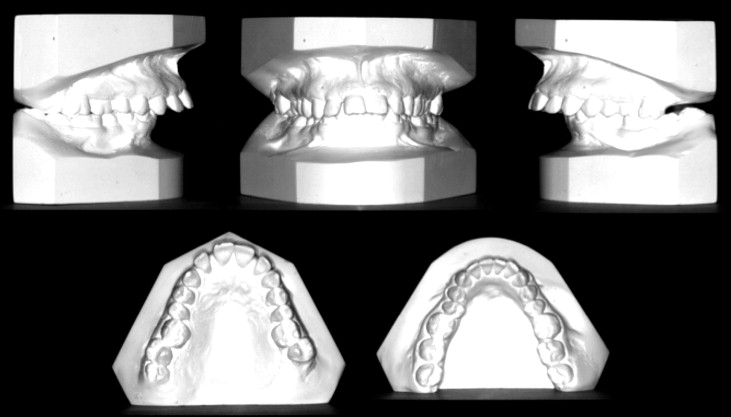
The patient had a symmetrical, brachyfacial face ( Fig 1 ). The profile was convex with a retrognathic mandible. There was an increased labiomental fold of the lower lip because of the increased overbite and diminished lower anterior face height. The chin-throat angle was ill-defined. When she smiled, large buccal corridors were visible.

The patient had a Class II Division 1 malocclusion ( Fig 2 ). On both sides, the molars and the canines were in Class II relationships. There were a severe, 7-mm overbite and an overjet of 13.5 mm. Buccal crossbites existed bilaterally at the level of the first and second maxillary premolars, as well as at the level of the maxillary right third molar. The maxillary dental midline was deviated 1 mm to the left, and the mandibular dental midline was deviated 1 mm to the right. The maxillary dental arch was tapered and constricted, especially in the first molar area; the mandibular dental arch was also narrow, with lingual positioning of the mandibular second premolar. The curve of Spee was accentuated, and the maxillary and mandibular incisors were proclined, most marked in the maxillary central incisors. There were diastemas between the maxillary central and lateral incisors bilaterally.
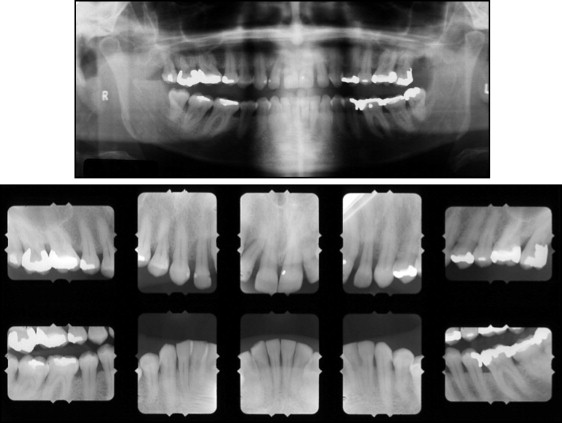
The patient’s periodontal status was healthy, with an adequate band of attached gingiva and no discernible dental mobility. Oral hygiene was adequate. Moderate generalized bone loss was observed and confirmed by radiology, indicating a past history of active periodontitis. A periodontist confirmed the current healthy and stable status of the periodontium.
All permanent teeth were present except for the maxillary left third molar. Extensive restorations were present on the maxillary and mandibular posterior teeth. The condyles were symmetrical and appeared normal. No pathology was noted ( Fig 3 ).
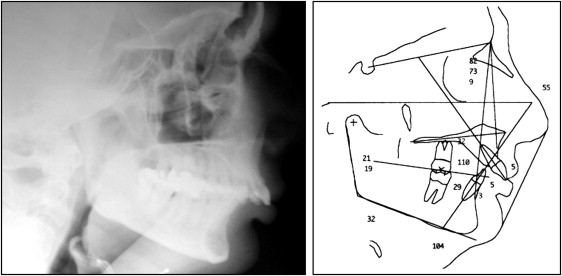
The patient had a severe Class II skeletal malocclusion with a retrognathic mandible and a hypodivergent pattern ( Fig 4 ; Table ). According to the analysis of Steiner, the maxilla was normally related to the cranial base (SNA, 82.5°), whereas the mandible was severely retrognathic (SNB, 72.6°; normal, 80°; ANB, 10°). The McNamara analysis indicated that the maxilla was slightly smaller than average (87.5 mm, average 91.0 mm). The effective length of the mandible was much shorter than average (97 mm, average 120 mm). The maxillomandibular difference was 9.8 mm (average 29.2 mm).
| Measurement | Standard | Initial | Final |
|---|---|---|---|
| SNA angle (°) | 82 | 82.5 | 81 |
| SNB angle (°) | 80 | 72.6 | 73 |
| ANB angle (°) | 2 | 9.9 | 8 |
| Wits (mm) | 1 | 11.6 | 6 |
| SN-Go-Gn (°) | 32 | 30.2 | 33.5 |
| MP to FH (°) | 25 | 19 | 21 |
| U1 to NA (°) | 22 | 22 | 10 |
| U1 to NA (mm) | 4 | 2.4 | 0.5 |
| L1 to NB (°) | 25 | 23 | 37 |
| L1 to NB (mm) | 4 | 4.4 | 8.5 |
| L1 to MP (°) | 90 | 104 | 111 |
| U1 to L1 (°) | 130 | 125 | 124 |
| Pog to NB (mm) | 1 | 0 | 3 |
The mandible was shorter than average (97 mm; normal, 107 mm). The maxillomandibular difference was 7.5 mm (average, 22.4 mm). The Wits appraisal was 11.6 mm (average, 1.1 mm). The patient had a low mandibular plane angle (19°). The maxillary and mandibular incisors were proclined.
Treatment alternatives
Because this patient was an adult with no clinically significant growth potential to assist in establishing the treatment goals with orthodontics alone, orthognathic surgery was proposed. Although this approach would allow for the correction of the skeletal discrepancy, achieve an ideal occlusion, and maximize the esthetic result, she refused the surgical plan. The remaining options included the following.
- 1.
Extract the maxillary first premolars to reduce the overjet and improve the canine relationship. However, this would only reduce the protrusion of the maxilla without affecting the position of the mandible.
- 2.
Extract the maxillary second molars and retract all maxillary teeth to establish a Class I relationship. This would also be a lengthy procedure.
- 3.
Use Class II mechanics without extractions; if unsuccessful, extract the first premolars, but this would steepen the occlusal plane and procline the mandibular anterior teeth even farther.
After extensive discussions with the patient, the nonextraction approach was selected.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


