A woman with an Angle Class III malocclusion and bilateral posterior crossbites complaining of difficulty in chewing was treated orthodontically without surgery. The treatment comprised asymmetric extractions, a removable mandibular lingual arch constriction appliance to narrow the mandibular arch, and a standard edgewise appliance to align the teeth. Pretreatment, posttreatment, and 1-year follow-up records are shown. With this treatment strategy of constricting the mandibular arch by using a combination of removable and fixed orthodontic appliances, we achieved a good result with optimal occlusion.
Posterior crossbite is a common problem in orthodontic practice and has been reported to occur in 8% to 22% of orthodontic patients. Posterior crossbite occurs when the buccal cusps of the maxillary posterior teeth occlude lingually to the buccal cusps of the corresponding mandibular teeth. The origin and basic mechanisms of posterior crossbite remain unclear, but various combinations of dental, skeletal, and neuromuscular functional components are known to be etiologic factors. The most common cause, however, is a posterior transverse discrepancy due to reduced maxillary dental arch width alone or combined with increased mandibular arch width.
The management of a posterior crossbite is based on the cause of the discrepancy between the maxillary and mandibular arch widths. Treatment usually involves the use of a maxillary expansion appliance, which can take many forms. The recommended treatment for younger patients is expansion of the maxillary arch with a removable expansion plate or a quad-helix appliance after grinding the occlusal interferences. If, however, the posterior transverse discrepancy is caused by increased mandibular arch width only or combined with reduced maxillary arch width, it is difficult to achieve the desired effect with fixed appliances and a maxillary expansion appliance. Orthodontists have tried to reduce maxillary arch width, but the reduction of mandibular arch width rarely has been reported.
The purpose of this article was to present an adult with bilateral posterior crossbites and an excessively wide mandibular arch treated orthodontically by using a removable mandibular lingual arch constriction appliance and fixed orthodontic appliances to reduce the mandibular arch width and correct the posterior transverse discrepancy.
Diagnosis and etiology
A 24-year-old woman was referred for orthodontic consultation. Her chief complaint was inability to chew well because her posterior teeth were not in contact properly when eating. This was a longstanding problem. The extraoral examination showed that she had a straight profile with a symmetric face and competent lips ( Fig 1 ). Functional examination showed no abnormal features. Intraorally, she had Class III molar and Class I canine relationships bilaterally, an anterior crossbite involving the maxillary lateral incisors, and a bilateral posterior crossbite involving the premolars and molars ( Fig 2 ).

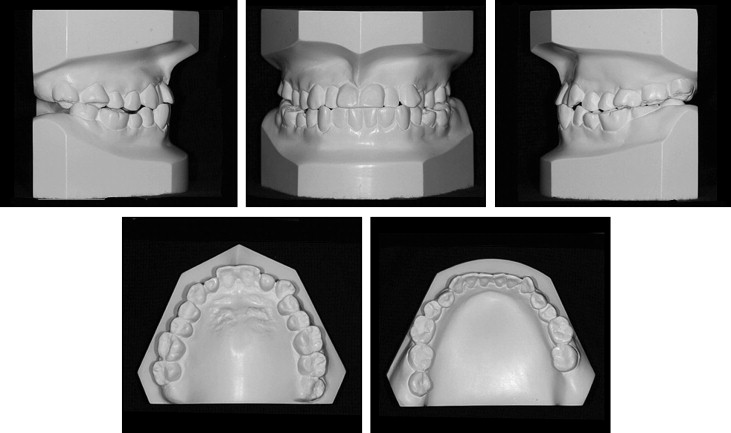
Both arches were U-shaped with mild crowding in the posterior segments. The posterior crossbite was due to an absolute maxillary to mandibular arch width discrepancy. The maxillary intermolar width between the central fossae of the right and left first molars was 54 mm, and the mandibular intermolar width between the mesiobuccal cusps of the left and right first molars was 58 mm. The maxillary molars were inclined buccally, and the mandibular molars were tipped lingually. The mandibular arch had a moderate curve of Spee. The maxillary midline was coincident with the facial midline, but the mandibular midline was deviated 1 mm to the left. Both maxillary lateral incisors were small.
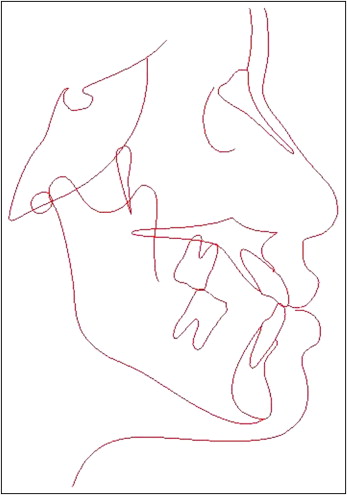
The panoramic radiograph showed all teeth present except the mandibular right third molar, which was impacted. The patient had a large amalgam restoration in the mandibular left second molar, 2 ceramic restorations in the maxillary right molars, and mild generalized periodontal bone loss, but no active periodontal disease ( Fig 3 ). The cephalometric tracing showed a skeletal Class I jaw relationship ( Fig 4 , Table I ). The patient was in good general health with no history of major systemic diseases.

| Measurement | Pretreatment | Posttreatment | Normal mean ± SD (Chinese adult) |
|---|---|---|---|
| SNA (°) | 85.5 | 85.5 | 81.69 ± 2.54 |
| SNB (°) | 84.5 | 84.1 | 78.94 ± 2.19 |
| ANB (°) | 1 | 1.4 | 2.75 ± 1.16 |
| U1 to NA (mm) | 6.6 | 7.1 | 5.56 ± 3.6 |
| U1 to NA (°) | 28.5 | 28.1 | 23.26 ± 6.17 |
| L1 to NB (mm) | 7.3 | 5.8 | 5.76 ± 2.29 |
| L1 to NB (°) | 24.8 | 25.1 | 27.38 ± 4.74 |
| Interincisal angle (°) | 125.7 | 125.5 | 123.22 ± 6.18 |
| MP:SN (°) | 33.6 | 33.5 | 32.85 ± 4.21 |
| FMIA (°) | 66.8 | 63 | 54.6 ± 6.5 |
Treatment objectives
The treatment objectives were to correct the anterior crossbite, eliminate the bilateral posterior crossbite by reducing mandibular arch width, resolve the crowding in the maxillary and mandibular arches, correct the mandibular midline deviation, and achieve a normal occlusion with ideal overjet and overbite while maintaining the straight pretreatment facial profile.
Treatment objectives
The treatment objectives were to correct the anterior crossbite, eliminate the bilateral posterior crossbite by reducing mandibular arch width, resolve the crowding in the maxillary and mandibular arches, correct the mandibular midline deviation, and achieve a normal occlusion with ideal overjet and overbite while maintaining the straight pretreatment facial profile.
Treatment alternatives
We considered that extraction of some mandibular teeth would be required to allow constriction of the mandibular arch to correct the bilateral posterior crossbite and to allow correction of the anterior crossbite. Two alternatives were considered and presented to the patient.
- 1.
Extraction of the mandibular second premolars. This would facilitate easier correction of the posterior crossbites and the anterior crowding but would involve extraction of a healthy tooth on the left side and leave behind a poorly restored second molar.
- 2.
Extraction of the mandibular right second premolar and left second molar. This extraction pattern would provide enough room to retract the posterior teeth, correct the crossbites, and avoid extracting a healthy tooth in the mandibular left quadrant where there was a poorly restored tooth.
The impacted maxillary right molar was to be surgically removed with both options. The patient chose the second plan comprising extraction of the mandibular right second premolar and left second molar, and surgical removal of the impacted molar.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


