Dentinogenesis imperfecta is an inherited dentinal dysplasia involving several risks for orthodontic treatment. This case report describes the multidisciplinary treatment of a 17-year-old girl whose Class II Division 1 malocclusion was complicated by dentinogenesis imperfecta type II and maxillary anterior trauma.
Dentinogenesis imperfecta (DI) is an inherited disorder of tooth development. Affected teeth are discolored and weaker than normal. The disorder is divided into 2 types. Type I is associated with a collagen defect, and type II is caused by a disorder of dentin mineralization. Therefore, type II is not associated with generalized conditions such as osteogenesis imperfecta (OI). For the successful treatment of patients with DI, not only is a differential diagnosis between types I and II necessary, but also a multidisciplinary approach should be considered. This case report illustrates the multidisciplinary treatment of a patient with type II DI, delineating some therapeutic guidelines for orthodontic management.
Diagnosis and etiology
A 17-year-old girl was referred to the department of orthodontics in KyungHee University Medical Center after she had received emergency treatment of resin-wire splinting on her maxillary incisors due to the trauma. Her chief complaints were unsightly discoloration of the teeth and maxillary incisor protrusion. Her family history supported the provisional diagnosis of DI, with a pedigree that spanned 2 generations on her maternal side. Her mother had undergone full-mouth rehabilitation because of DI, and therefore wanted her daughter to have prosthetic reconstruction as her final treatment. The patient was in good physical condition. Her medical history showed no evidence of OI, such as a history of frequent fractures of long bones, laxity of joints, blue sclera, hearing loss, or increased bleeding tendency.
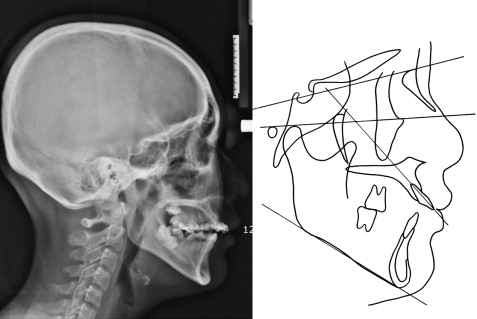
Pretreatment photographs ( Fig 1 ) showed a dentition with brown to gray opalescent teeth without severe attrition. She had a Class II Division 1 malocclusion with crowding, anterior open bite, large overjet, palatally blocked maxillary left second premolar, and multiple caries. Dental casts confirmed asymmetric right and left occlusal curves caused by the extrusion of maxillary right first molar ( Fig 2 ). A panoramic radiograph showed impaction of the mandibular left second molar and the 4 third molars in addition to the features of DI: short roots, bulbous crowns, cervical constrictions, and pulpal obliteration ( Fig 3 , A ). In the periapical film, tooth fractures on both maxillary central incisors were confirmed without alveolar bone fracture ( Fig 3 , B ). A lateral cephalometric radiograph and its tracing showed a skeletal Class II hyperdivergent pattern ( Fig 4 ).



Treatment objectives and plan
Integrated conservative, orthodontic, periodontal, and prosthodontic treatment objectives were established as shown in Table I . The ultimate objective was to achieve an esthetic reconstruction to conceal the discoloration. Full-coverage restorations were planned except for the posterior teeth, because this patient had neither severe attrition nor reduced vertical dimension.
| Conservative objectives | Restore carious teeth Follow up the traumatized teeth |
| Orthodontic objectives | Improve facial and dental esthetics Retrude maxillary anterior teeth and upper lip Maintain sagittal position of the mandibular incisors Decrowd the dentition Level the asymmetric occlusal curve Establish Class I canine and Class II molar relationships Obtain functional occlusion by proper overjet and overbite |
| Periodontal objectives | Detach the heavy labial frenum Lengthen the crown of the substituted tooth Replace the hopeless mandibular first molar with an implant |
| Prosthodontic objectives |
Improve the dental esthetics; reconstruct the discolored teeth Establish the final occlusion Maintain the vertical dimension |
The specific objectives of orthodontic treatment included retrusion of the maxillary anterior teeth and upper lip, maintenance of the sagittal position of the mandibular incisors, alignment of the maxillary and mandibular teeth, vertical control of the asymmetric occlusal curve, and establishment of a Class II molar relationship with proper overjet and overbite. The orthodontic treatment plan involved extraction of the fractured maxillary central incisors, the maxillary left second premolar, the hopeless mandibular right first molar, the impacted mandibular left second molar, and the 4 third molars. To preserve the alveolar ridge, extractions of the maxillary left central incisor and the mandibular right first molar were postponed until they were replaced by prostheses. The maxillary right lateral incisor, canine, and first premolar would substitute for the maxillary right central incisor, lateral incisor, and canine, respectively.
Treatment objectives and plan
Integrated conservative, orthodontic, periodontal, and prosthodontic treatment objectives were established as shown in Table I . The ultimate objective was to achieve an esthetic reconstruction to conceal the discoloration. Full-coverage restorations were planned except for the posterior teeth, because this patient had neither severe attrition nor reduced vertical dimension.
| Conservative objectives | Restore carious teeth Follow up the traumatized teeth |
| Orthodontic objectives | Improve facial and dental esthetics Retrude maxillary anterior teeth and upper lip Maintain sagittal position of the mandibular incisors Decrowd the dentition Level the asymmetric occlusal curve Establish Class I canine and Class II molar relationships Obtain functional occlusion by proper overjet and overbite |
| Periodontal objectives | Detach the heavy labial frenum Lengthen the crown of the substituted tooth Replace the hopeless mandibular first molar with an implant |
| Prosthodontic objectives |
Improve the dental esthetics; reconstruct the discolored teeth Establish the final occlusion Maintain the vertical dimension |
The specific objectives of orthodontic treatment included retrusion of the maxillary anterior teeth and upper lip, maintenance of the sagittal position of the mandibular incisors, alignment of the maxillary and mandibular teeth, vertical control of the asymmetric occlusal curve, and establishment of a Class II molar relationship with proper overjet and overbite. The orthodontic treatment plan involved extraction of the fractured maxillary central incisors, the maxillary left second premolar, the hopeless mandibular right first molar, the impacted mandibular left second molar, and the 4 third molars. To preserve the alveolar ridge, extractions of the maxillary left central incisor and the mandibular right first molar were postponed until they were replaced by prostheses. The maxillary right lateral incisor, canine, and first premolar would substitute for the maxillary right central incisor, lateral incisor, and canine, respectively.
Treatment alternatives
Our treatment plan involved atypical extractions. In the maxillary arch, another option would have been to extract the right and left first premolars to reduce the anterior protrusion and overjet. However, on the right side, extraction of the first premolar would decrease the number of remaining teeth and require additional implant surgery for the lost central incisor. Orthodontic traction of the palatally blocked left second premolar into the extracted first premolar site would have a periodontal advantage, but we needed reinforced anchorage on the left side so as not to deviate the upper midline to the right during the mesial movement of right lateral incisor, canine, and first premolar.
In the mandibular arch, surgical exposure and orthodontic traction of the impacted left second molar seemed to be reckless, because of its poor direction and position. Implants or prosthetic reconstructions for lost second molars would have been unnecessary considering the Class II molar relationship as the final occlusion.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


