A detailed clinical examination is important for early diagnosis of oral lesions in every dental specialty, including orthodontics, particularly because these patients are constantly checked during orthodontic treatment. This report describes 2 men receiving orthodontic treatment and who had swelling on the hard palate diagnosed as mucoepidermoid carcinoma. Both patients received appropriate treatment and had a good prognosis because of the rapid recognition of these oral lesions by their orthodontists.
In dentistry, whatever the specialty, clinicians must be able to recognize normal oral structures, variations of normality, and lesions. The oral cavity is accessible, and most oral lesions can be easily identified. Salivary-gland tumors are relatively uncommon; consequently, a substantial number of these lesions are diagnosed as advanced disease. Mucoepidermoid carcinoma (MEC) is the most common malignant tumor of the major and minor salivary glands in adults and children.
The prognosis of patients with MEC depends on several factors such as histologic grade, staging of the tumor, invasion, and involvement of adjacent structures. According to this information, it is possible to estimate the risks of recurrence and death. It is well known that patients with low-grade malignant tumors detected at the initial clinical stage have a better prognosis than do patients with advanced disease. However, several oral lesions, including malignant tumors, can be asymptomatic and thus delay an early diagnosis.
Case report 1
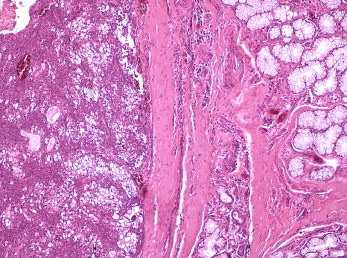
A 31-year-old man was referred to the oral diagnosis clinic of Piracicaba Dental School of the University of Campinas in Brazil by his orthodontist for evaluation of a painless swelling on the hard palate. The patient reported that the lesion had been present for about 2 months. On oral examination, swelling on the right side of the hard palate was observed. The swelling was soft and circular, measuring approximately 1.0 × 0.8 cm at its maximum dimension ( Fig 1 ). No regional lymph node enlargement was detected in the extraoral examination. The panoramic radiograph showed no bone alteration. An incisional biopsy was taken, and the histopathologic analysis showed a glandular neoplasm composed of cellular proliferation of mucous, epidermoid, and intermediate cells with a prominent intracystic space, establishing the diagnosis of low-grade mucoepidermoid carcinoma ( Fig 2 ). The patient was referred to a head and neck surgeon, who performed a wide local excision with adequate tumor-free margins. The patient has been in follow-up for about 5 years without signs of recurrence or metastasis ( Fig 3 ).


Case report 2
Similarly, a 30-year-old man was referred by his orthodontist for analysis of a lump on the palate. During the intraoral examination, the swelling was observed on the left side of the hard palate with bluish coloration; it measured 1.2 cm in diameter ( Fig 4 ). The patient reported that he did not know about the lesion, but sometimes he felt an itch on the palate. No regional lymph node enlargement was detected, and the panoramic x-ray showed no bone involvement. An incisional biopsy was performed, and the histopathologic analysis was compatible with low-grade mucoepidermoid carcinoma. Perineural invasion and mitotic figures were absent. The patient was referred to a head and neck surgeon, who surgically removed the tumor. The patient has been in follow-up for about 2 years, and no signs of recurrence or metastasis have been observed.



