Introduction
As computer-assisted surgical design becomes increasingly popular in maxillofacial surgery, recording patients’ natural head position (NHP) and reproducing it in the virtual environment are vital for preoperative design and postoperative evaluation. Our objective was to test the repeatability and accuracy of recording NHP using a multicamera system and a laser level.
Methods
A laser level was used to project a horizontal reference line on a physical model, and a 3-dimensional image was obtained using a multicamera system. In surgical simulation software, the recorded NHP was reproduced in the virtual head position by registering the coordinate axes with the horizontal reference on both the frontal and lateral views. The repeatability and accuracy of the method were assessed using a gyroscopic procedure as the gold standard.
Results
The interclass correlation coefficients for pitch and roll were 0.982 (0.966, 0.991) and 0.995 (0.992, 0.998), respectively, indicating a high degree of repeatability. Regarding accuracy, the lack of agreement in orientation between the new method and the gold standard was within the ranges for pitch (−0.69°, 1.71°) and for roll (−0.92°, 1.20°); these have no clinical significance.
Conclusions
This method of recording and reproducing NHP with a multicamera system and a laser level is repeatable, accurate, and clinically feasible.
Highlights
- •
A new method was used to record and reproduce natural head position.
- •
The method was based on multicamera system and a laser level.
- •
The reliability and viability were evaluated via studies on physical model.
- •
The method was highly reproducible.
- •
Its accuracy was higher than 2 degrees.
Natural head position (NHP) is the most reproducible relaxed head position adopted by a subject looking horizontally into infinity. Two methods are described to determine NHP in the clinic. The first method asks the patient to look into horizontal infinity, and second method asks the patient to look into his or her own eyes in a mirror. Physiologically, head position is controlled by vestibulo-ocular and vestibulospinal reflexes, as well as by inner ear otolithic gravitational responses that provide interactions among eye position, head position, and muscles. According to previous studies, NHP can be influenced by nasorespiratory function, occlusion, craniofacial skeletal morphologic features, and visual feedback deprivation. Based on these findings, NHP might change with different emotional states, ages, personal characteristics, environmental conditions, and cervical discomfort.
Since NHP provides a coordinate reference system for taking measurements and therefore has vital importance for diagnosis, surgical design, postoperative outcome evaluation, and developmental tracking in patients with dentomaxillofacial deformities, it has gained the interest of many experts. Previous studies have mainly focused on how to record NHP 2 dimensionally. Now, with the development of computer-assisted surgical design, many authors are using new methods for recording 3-dimensional (3D) NHP and integrating it into a computer-assisted surgical design protocol.
Schatz and Xia et al conducted a series of studies on how to record and reproduce NHP 3 dimensionally using a gyroscope. According to our experience, this method is accurate and feasible for preoperative design but impractical for postoperative evaluation and long-term follow-up. The main reason for this limitation is that in the gyroscopic procedure, recording and reproduction are based on the alignment between the patient’s occlusion and the gyroscope, and when the occlusion is altered after surgery, the alignment is also changed. As a consequence, the entire procedure, including the computed tomography (CT) scan, must be repeated at each follow-up visit, with an unacceptable increase in radiation exposure. Other disadvantages of the gyroscopic procedure include (1) the requirement for specialized software and equipment such as a bite-jid, facebow, and acrylic materials; and (2) the total weight of the gyroscope that might affect head orientation because the weight is in front of the center of gravity.
Weber first reported the method of recording NHP using a stereophotographic system. In that study, the true vertical and horizontal laser lines were projected for orientation and then were marked on the patient’s face with ink dots. Using a 3D camera system, photographs were taken to capture the orientation of the reference points. Compared with the gyroscope and the procedure of Schatz and Xia et al, Weber’s method has the following advantages: (1) no special devices and software, (2) no occlusion alignment, and (3) no radiation exposure.
However, there is some uncertainty about the accuracy and convenience of the method of Weber for 2 reasons. First, since head posture can be affected by visual motion, when doctors draw marking dots according to laser lines, patients may be distracted and move their head slightly. Second, the separate procedure of reference marking and taking 3D photographs will inconvenience both patients and doctors.
We modified the method of Weber by capturing laser reference lines and the patient’s face together, eliminating the marking of reference dots. This study was designed to test the accuracy and repeatability of this new technique. Since several variables can affect NHP, such as personal characteristics, environmental conditions, room heat, and a person’s excitation state, this study was based on a physical model to eliminate other factors outside the technique itself.
Material and methods
A physical head model (Brainlab, Munich, Germany) made from CT-compatible plastic material was used in the study. A digital gyroscope (3DM; MicroStrain, Williston, Vt) assembled with a facebow and reference markers (Medical Modeling, Golden, Colo) was fixed to the physical model by 2 titanium screws at each side to ensure a solid alignment between the gyroscope and the model throughout the study. A CT scan was acquired with a cone-beam CT scanner (VG; NewTom, Verona, Italy). The scanning matrix was 400 × 400 with a depth of gray level of 16 bits. The layer thickness was 0.075 mm with a field of view of 15 cm. The position of the model was recorded by the gyroscope simultaneously with the CT scanning. Data in DICOM format were transferred into Proplan CMF virtual design software (Materialise, Oberdorf, Switzerland). A virtual image of the model and the gyroscope assembly was obtained by surface rendering reconstruction of the DICOM data. The original coordinate system of the CT scan was quoted by the software, which was recorded by the gyroscope.
NHP was recorded by capturing a 3D image of the physical model with horizontal lines projected onto it by the laser level. The procedure was as follows.
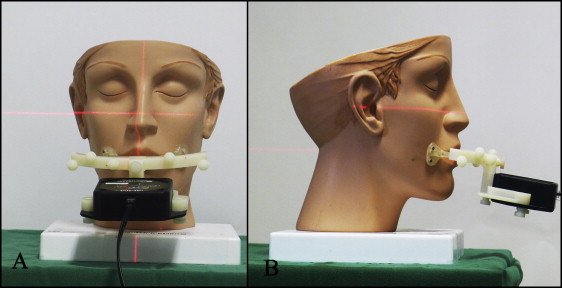
First, a laser level (SaiWei, Shanghai, People’s Republic of China) was used to project a horizontal line onto the physical model. As stated in the manufacturer’s handbook, the wavelength of the laser beam was 635 to 670 nm, and the horizontal accuracy was 0.2 mm when the distance was 1 m. The distance between the physical model and the laser level in our test was 1.5 m. The laser level was set up in front of the model to enable the horizontal line to be projected across the entire face ( Fig 1 ).
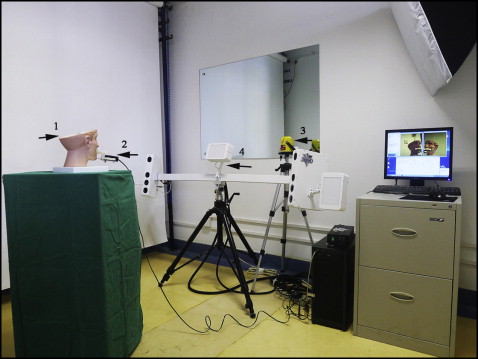
Second, a 3D image was obtained using a multicamera system (3dMD, Atlanta, Ga). This stereophotography unit uses 4 cameras, 2 of which are positioned on each side of the subject. It achieves a 180° face capture (ear to ear), with a capture speed of 1.5 ms and a resolution of 400 dpi. The reported accuracy in the manufacturer’s handbook is 1.5% of the total observed variance. The center flashlight of the multicamera system was turned off so that the laser beam reference line appeared more clearly on the obtained images. The instruments and imaging environment are shown in Figure 2 .
Because the 3D image captured the model from ear to ear, the horizontal reference line could be used to record both the pitch and roll orientations simultaneously. The frontal view was used to record the roll and the lateral view to record the pitch ( Fig 3 ).
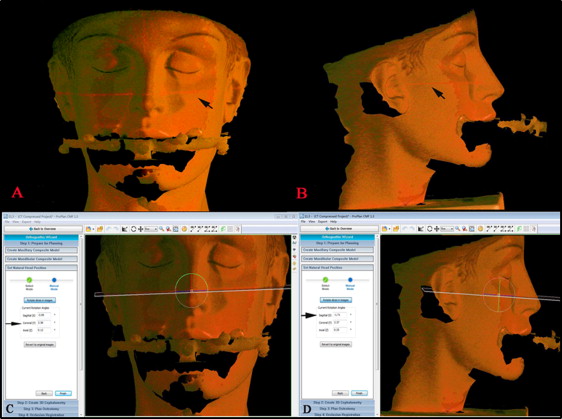
NHP was reproduced in the virtual model by altering the virtual head position until the both vertical and sagittal vectors coincided with the horizontal reference line. The procedure was as follows.
- 1.
The 3D camera image was saved in .wrl format and imported into the surgical design software.
- 2.
The 3D image and the CT scan were superimposed through a surface registration procedure, with the CT scan set as the fixed object and the 3D image as the floating object.
- 3.
The virtual head position was moved manually according to the horizontal laser beam line on the 3D image. In the virtual environment, the x-axis represents the horizontal vector, the y-axis represents the vertical vector, and the z-axis represents the sagittal vector. In this sense, pitch, yaw, and roll refer to the angles around these 3 axes, respectively. Thus, the x-axis coordinate was parallel to the line on the frontal view; simultaneously, the z-axis coordinate was parallel to the line on the lateral view ( Fig 3 ).
- 4.
The coordinate axis was double-checked from both views. The changes in the pitch and roll angles during the movement were recorded.
We used a gold standard for NHP recording and reproduction. The orientation of each head position was recorded by the digital gyroscope, by recording the pitch and roll angles simultaneously. The pitch and roll alterations between 1 test head position and the head posture during the CT scan were calculated. These alterations were the angles that needed to be applied when reproducing a recorded head position on the virtual model and were considered the gold standard.
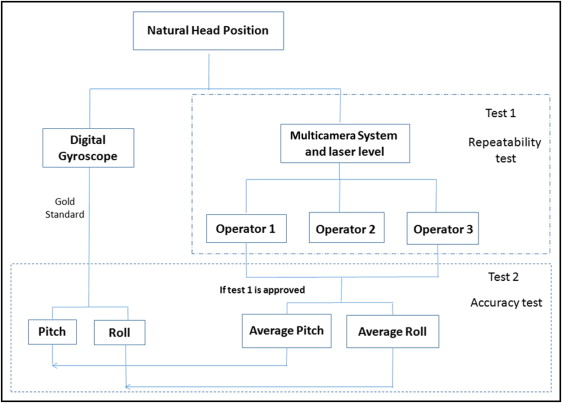
This study was designed to answer 2 questions: (1) whether the results obtained with the new method depend on operator experience, and (2) whether the new method is as accurate as the gyroscopic method. Two tests were therefore used: the first to assess the repeatability of the new method among different operators, and the second to assess its accuracy.
For the repeatability tests, a minimum sample of 33 participants would yield an expected intraclass correlation coefficient (ICC) of 0.9 and a lowest acceptable ICC of 0.8 for 3 repetitions per participant. For the accuracy tests, the total sample size of 35 was determined before the study based on an expected difference of 2 between measurements and the gold standard. This sample size would yield an alpha of 0.05 and a power of 0.80.
During the recording procedure, the physical model was randomly oriented 35 times so that 35 pairs of data were obtained, comprising both the corresponding angles recorded by the multicamera system and the laser level, and the angles recorded by the gyroscope. During the reproduction procedure, 3 experienced orthognathic surgeons (X.-j.L., Z.-l.L., and another) independently registered the virtual head. The resultant pitch and roll angles were recorded. The experimental design is shown in Figure 4 .