The purpose of this article is to present a long-term follow-up of the growth of the face and the nasomaxillary complex in a pair of identical twins, one of whom had suffered severe midfacial trauma at age 2 years. Growth of the face and the nasomaxillary complex was longitudinally assessed and compared by means of facial photographs and cephalometric x-rays. Twin A suffered Le Fort II and III fractures with an associated frontal bone injury in early childhood and subsequently developed significant midface hypoplasia; twin B had no trauma and normal facial growth and development. Facial profile difference between the twins gradually became more pronounced until age 19. Twin A had obvious retrusion of the midfacial region, including the nasal bones on visual examination and radiographic study. At age 20, she underwent orthognathic surgical correction of the traumatic deformity. Her unaffected sibling, twin B, provided the genetic facial phenotype for the surgical orthognathic reconstruction.
Pediatric trauma patients admitted to the hospital have a 5% incidence of facial fractures. Although midface trauma occurs in children, it seems to be rare. There is surprisingly little information in the literature regarding the long-term effects of trauma to the midface in early childhood.
Pediatric trauma patients differ from their adult counterparts. Patterns of injury, treatment algorithms, and potential consequences of facial trauma and its treatment are affected by the physiology of facial growth and development. Knowledge of facial growth and development is important in understanding patterns of pediatric facial trauma and the rationale behind its treatment. Changes in facial shape and the development of the sinuses and dentition play crucial roles in the fracture patterns of pediatric patients.
Midfacial growth and development have been shown in animal studies to be intimately related to the cartilagenous nasal septum. Traumatic deformity of the cartilaginous septum is related to later underdevelopment of the cartilaginous middle third of the nose and disturbed maxillary growth. Demonstrating this relationship in humans has been more difficult and requires long-term follow-up studies to evaluate nasal and maxillary growth. Many studies relate retrospectively traumatic events to later abnormal growth, yet do not provide clear relationships between the environment and genetics.
In the study by McCoy et al of 1500 facial fractures, 64 patients were children, and only 55% of the fractures involved the midface area. They stated, “on the basis of this series a properly reduced and stabilized facial fracture had no adverse effect on the growth of the facial bones.” One documented case of growth disturbance with midface fractures was found: a patient with delayed treatment of a nasoethmoidal fracture. Converse and Dingman, discussing nasomaxillary fracture in children, stated that midfacial fracture might explain nasal deviation and nasomaxillary hypoplasia that otherwise has no apparent cause. They further stated that “underdevelopment, maldevelopment, malocclusion and ankylosis are all potential complications of the facial bone fractures in children.” They made no specific statement about the location or degree of midfacial growth deficiency or how their opinion was derived.
The etiology of Class III malocclusion is generally believed to be genetic. Many environmental factors have been suggested as contributing to the development of Class III malocclusion. Twin studies have been beneficial in separating genetic and environmental influences on facial growth and malocclusion. In a review of the literature, we found only 1 study of identical twins in which one sustained a traumatic injury to the midfacial region at a young age. Grymer and Bosch reported that 1 twin had a septal abscess at age 7 with a subsequent defect in the middle inferoposterior septum. At age 17, the affected twin had a more retruded maxilla that was also shortened vertically in the anterior region. The nasal bone was also retruded. However, total facial vertical height was the same.
The aim of this study was to assess and compare longitudinally the growth of the face and the nasomaxillary complex in a pair of identical twins, one of whom had severe midfacial trauma at age 2. The trauma included Le Fort II and III fractures with an associated frontal bone injury, which subsequently resulted in significant midface hypoplasia; the unaffected twin had no trauma and normal facial growth and development.
Case report
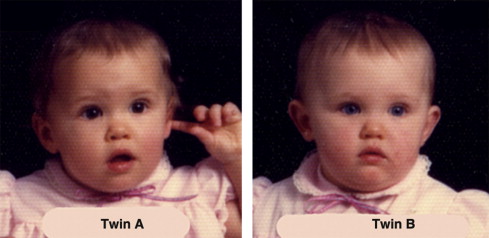
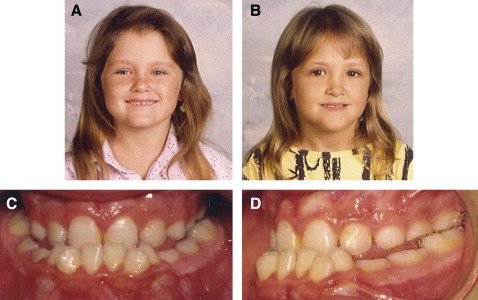
A girl, age 15 years, sought treatment for a facial deformity. She had an identical twin sister ( Fig 1 ). The patient, twin A, had a well-documented history of midfacial trauma at age 2, when a wooden bed frame fell on her face, causing Le Fort II and III fractures with an associated frontal bone injury. She was treated at that time by an open reduction with internal wire fixation of the fractures. She was subsequently followed by the same orthodontist. Facial growth disturbance was noted at age 6, and bilateral posterior and anterior crossbites were evident ( Fig 2 ). The facial growth disturbance became more prominent with growth, and orthodontic treatment was started at age 9 years. Dental development and maxillary molar and premolar eruption were also disturbed because of the Le Fort II and III fractures and subsequent surgery in early childhood. The deciduous molars were overretained, and deviated premolar tooth bud positions and failure of eruption were noted on both sides. The eruption of the maxillary second molar was also delayed. During the orthodontic treatment, the deciduous molars were extracted, and the maxillary premolars were surgically exposed and orthodontically extruded into the arch. The right first and third molars and the left second and third molars were extracted during the leveling and alignment phase of the maxillary dental arch. Nevertheless, the facial profile difference between the twins gradually became more pronounced ( Figs 3 and 4 ). Twin A had obvious midface retrusion, including the nasal bones, with a Class III malocclusion, a negative overbite of 9 mm, and enlarged facial height.


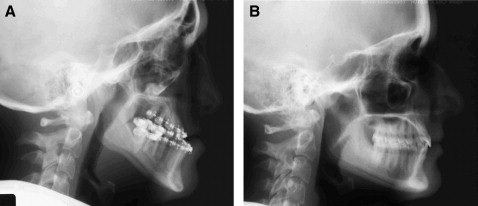
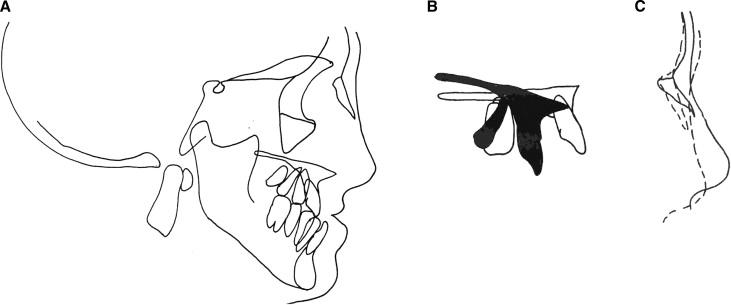
Radiographic studies including lateral and posteroanterior cephalometric and panographic images where obtained at intervals during growth and development. A cephalometric radiograph was taken at age 19, after the presurgical orthodontic preparation phas ( Fig 5 , A ). This treatment procedure prepared the maxillary and mandibular dental arches to achieve stable occlusal relationships postoperatively. It included expansion of the maxillary and mandibular arches, leveling and alignment of both dental arches, and decompensation of the incisor positions—ie, protrusive inclination of the mandibular incisors and retrusive inclination of the maxillary incisors, creating an enlarged negative overjet of 12 mm. A cephalometric radiograph was also obtained of the unaffected twin ( Fig 5 , B ). The radiographs were analyzed with architectural and structural cephalometric analysis and compared between the twins ( Table ). Superimpositions of the cephalograms of the twins were used for comparison and surgical planning ( Fig 6 ).
| Twin A | Twin B | |
|---|---|---|
| Lateral cephalogram date | 8/22/2001 | 8/28/2001 |
| SNA (°) | 70.58 | 78.19 |
| SNB (°) | 75.53 | 76.69 |
| ANB (°) | −4.95 | 1.5 |
| Maxillary length, Co-A (mm) | 66.92 | 82.22 |
| Mandibular length Co-Gn (mm) | 102.04 | 105.75 |
| Pog to nasion vertical (mm) | −10.78 | −3.64 |
| Wits (mm) | −12.15 | 1.18 |
| FMA (°) | 33.36 | 21.34 |
| SN-mandibular plane (°) | 41.25 | 29.06 |
| Y-axis to S-N (°) | 71.78 | 67.63 |
| Y-axis to FH (°) | 63.89 | 59.91 |
| Post:ant face hgt S-Go:N-Me (%) | 58.28 | 64.93 |
| Lower height ratio L\T (%) | 58.04 | 56.74 |
| Maxillary 1 to SN (°) | 91.13 | 104.2 |
| Maxillary 1 to FH (°) | 99.01 | 111.91 |
| Maxillary 1 to NA (°) | 20.55 | 23.01 |
| Maxillary 1 to A-Pog (mm) | −1.68 | 3.29 |
| Mandibular 1 to mandibular plane (°) | 90.18 | 93.95 |
| Mandibular 1 to A-Pog (mm) | 6.14 | 1.86 |
| Mandibular 1 to NB (°) | 26.96 | 20.7 |
| Interincisal angle (°) | 137.44 | 132.79 |
| Nasolabial angle (°) | 100.99 | 94.22 |
| Upper lip protrusion (mm) | −10.28 | −6.55 |
| Lower lip protrusion (mm) | −2.04 | −4.99 |
At the age of 20 years, twin A underwent surgical correction of the traumatic deformity. The orthognathic surgery included a high Le Fort I osteotomy with maxillary advancement and impaction and cranial bone grafting associated with bilateral mandibular sagittal split osteotomy with setback and genioplasty. The final cephalogram and facial photos ( Fig 7 ) showed improvement in the anteroposterior and vertical proportions of twin A’s facial appearance.

Results
The similarity of facial appearance between these monozygotic twins at the age of 1 year, a few months before twin A’s traumatic episode, is shown in Figure 1 . Facial growth disturbance tendency was evident at 6 years ( Fig 2 ). Abnormal dental development and eruption sequence disturbance of the maxillary dentition were evident in the posterior segments as a trauma consequence. The differences in facial appearance between the sisters increased over time and were more pronounced at the age of 15 years, showing the progression of the influence of the trauma on maxillary and nasal growth and development. Twin A, who had the trauma, had a retrusive and underdeveloped nasomaxillary complex, reflected in a flattened midface. The vertical dimension of the face was enlarged in twin A with a vertical pattern of jaw growth. Cephalometric measurements from standardized lateral cephalograms taken in natural head position show skeletal and dentoalveolar differences between the twins as they developed until the orthognathic surgery. The SNA of twin A was 70.58°, and her effective maxillary size (Co-A) was 66.92 mm, whereas twin B had an SNA of 78.19° and a maxillary size of 82.22 mm. There were no great differences in mandibular size (Co-Gn) (twin A, 102.04 mm; twin B, 105.75 mm). Therefore, the difference found in ANB angle (twin A, –4.95°; twin B, 10.5°), and in the Wits appraisal might account for the differences in growth of the nasomaxillary complex. The differences in the vertical measurements between the twins are depicted in the FMA, SN to Mn plane, and y-axis indexes and indicate the vertical pattern of skeletal face growth in twin A. Although this cephalometric radiograph of twin A was taken after dentoalveolar orthodontic decompensation in preparation for orthognathic surgery, the dental measurements still indicate Class III features of incisor position with retroclined mandibular incisors and a tendency toward proclined maxillary incisors.
Twin A responded well physiologically and psychologically, and she was pleased with the treatment outcome. The improved facial esthetics and skeletal and dentoalveolar balance in twin A decreased the differences in facial appearance between the pair and dramatically increased their similarity.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


