Introduction
Our objectives were to investigate the prevalence, resorption location and extent, and potential risk factors for impacted canine-associated root resorption (ICARR) in Chinese patients, who, unlike white patients, have predominantly buccal maxillary canine impactions.
Methods
Pretreatment cone-beam computed tomography scans of 170 Chinese subjects (ages, 12-30 years; mean, 14.5 years) with impacted maxillary canines (101 buccal and 69 palatal impactions) and 170 age- and sex-matched subjects without impactions were used. All cone-beam computed tomography records were evaluated in software programs by 1 rater. The prevalence, location, and extent of ICARR at the maxillary lateral incisor, central incisor, and first premolar were analyzed. To identify risk factors for ICARR, the subjects with impacted canine were divided into 2 groups (with and without root resorption). Measurements of 10 variables were individually compared between the groups and then tested together by using binary logistic regressions for each tooth.
Results
Compared with the control subjects and the side of nonimpaction, root resorption was significantly more prevalent in the canine-impaction subjects and the side of impaction ( P <0.01), with overall prevalence rates of 27%,18%, and 10% at the maxillary lateral incisor, the central incisor, and the first premolar, respectively. Predominantly affecting the apical third of all teeth, ICARR, if present, reached the pulp of the maxillary lateral incisor, the central incisor, and the first premolar at rates of 36%, 57%, and 0%, respectively. Individually, variables reflecting the proximity to the impacted maxillary canine had different measurements ( P <0.05) between the impaction sites (maxillary quadrants) with and without root resorption for each tooth, whereas the canine development stage factor was only significant for the maxillary central and lateral incisors. No significant difference of ICARR prevalence was found between subjects with buccal and palatal impactions. Combined, the contact relationship was the dominant predictor for ICARR at all teeth, with “in contact” (<1 mm separation) having the largest and most significant increase of root resorption likelihood compared with “out of contact” (≥1 mm separation); odds ratios were 9.9, 3.7, and 5.9 for the maxillary lateral incisor, the central incisor, and the first premolar, respectively.
Conclusions
Maxillary canine impaction increases the risk of root resorption at adjacent teeth (incisors and first premolars). Physical proximity (<1 mm) between the impacted canine and an adjacent root is the most important predictor for root resorption, and this characteristic is largely similar in Chinese patients to that in white people.
Maxillary canines are the second most frequently impacted teeth, with general prevalence rates of 1% to 3%. Palatal impaction is more common in white people, and buccal impaction is more common in Asians. Untreated maxillary canine impaction can interfere with the alignment of neighboring teeth, shorten dental arches, and increase the chance of follicular cyst formation and recurrent infections. It can also cause external resorption of adjacent teeth, an irreversible damage that potentially leads to tooth loss.
Because of a general lack of symptoms and clinicians’ reliance on 2-dimensional radiographic imaging for diagnosis, impacted canine-associated root resorption (ICARR) has a tendency to be diagnosed late, in relation to both the patient’s age and the extent of resorption. Image enlargement, distortion, and structure overlap are common limitations of 2-dimensional radiograph techniques that reduce image quality and diagnostic accuracy. It has been reported that superimposition of an impacted canine crown on adjacent incisor roots on 2-dimensional radiographs obscured the root morphology in 45% of the teeth, and 37% of the lateral incisors affected by root resorption appeared normal on the 2-dimensional radiographs.
Recent advancements in computed tomography (CT) techniques, especially cone-beam CT (CBCT), have significantly improved the sensitivity and accuracy of the diagnosis of root resorption. Based on CT techniques, it was found that in white people, about 40% of the incisors adjacent to impacted canines had resorption, whereas in Asians, the prevalence rates of root resorption varied between 23% and 50%. ICARR in white patients happens predominantly in the middle third of the incisors, followed by the apical third, and rarely in the cervical third. In addition, about 60% and 43% of ICARR of the lateral and central incisors, respectively, had pulpal involvement. To date, it is unclear whether these ICARR features are shared by Asian patients.
Risk factors predisposing for root resorption in canine impaction patients have been studied with varying results. Except for 2 studies (female sex), most studies on white patients pointed to local factors, especially those directly involving the impacted canine. On 2-dimensional panoramic images, specific canine location (mesial to the midroot axis of the lateral incisor) and angulation (canine long axis to the midsagittal plane greater than 25°) were suggested to increase root resorption by 50%. On the other hand, based on 3-dimensional imaging techniques, several recent studies have emphasized the role of physical pressure or contact from the impacted maxillary canine.
In this study, we used 3-dimensional CBCT imaging techniques to investigate the prevalence, resorption location and extent, and predisposing risk factors for ICARR in a Chinese population. Age and sex, together with several local factors involving the impacted canine, were assessed as potential risk factors, and significant predictors for root resorption at the central and lateral incisors and the first premolars were identified.
Material and methods
Pretreatment CBCT scans of 170 Chinese patients with impacted maxillary canines (69 palatal and 101 buccal impactions) and 170 age- and sex-matched subjects without impactions were selected from a pool of patients seeking orthodontic treatment at the Nanjing Medical University Institute of Stomatology, Nanjing, China, between June 2010 and September 2011. The prestudy power analysis was based on the reported prevalence of root resorption with a hypothesis that canine impaction significantly increases root resorption at adjacent roots. With assumptions of 20% and 5% prevalence rates of root resorption in our canine-impaction and control samples, respectively, a minimum sample size of 49 was required for 80% power (calculated in G*Power, version 3) to detect root-resorption prevalence differences. Our samples with palatal (n = 69), buccal (n = 101), and combined (n = 170) impactions had power values of 92%, 98%, and 99%, respectively.
Sample inclusion criteria were patients (1) who were 12 to 30 years of age at the time of the CT scan and (2) with clinically diagnosed unilateral or bilateral maxillary canine impaction (impaction group). The exclusion criteria were previous orthodontic treatment, history of dental trauma or anterior maxillary dental surgery, and dental age younger than the late mixed dentition. Accessing and analyzing these records for this study was approved by the institutional review board of the Ohio State University.
All CBCT records were obtained with the patients in an upright position with the same CBCT machine (NewTom VG; QR srl, Verona, Italy) with the same settings: 16-cm-diameter field of view, 110 kV, 1-20 mA (pulsed mode), and 0.3-mm voxel size.
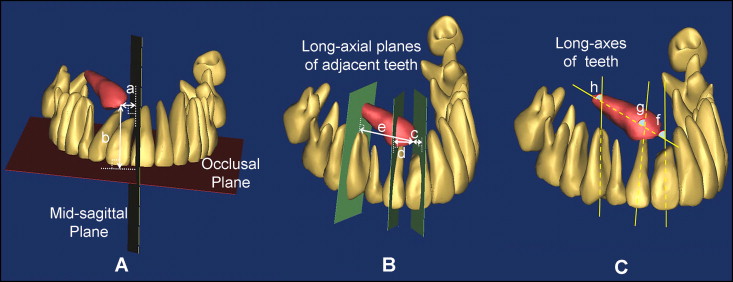
All CBCT records (DICOM files) were randomly coded, with patient identification information removed, and then analyzed by 1 rater (B.Y.). The DICOM files were first imported into Mimics software (version 13.0; Materialise NV, Leuven, Belgium) and segmented to display the teeth for 3-dimensional surface rendering at a Hounsfield unit range of 1300 to 3071. This range was chosen based on a pilot experiment of 20 patients that demonstrated consistency in tooth structure segmentation. Then the image was reoriented according to the protocol of Swennen to adjust the skull to a standard position. The landmarks related to the measurements were selected in the volumetric view by using the digitizing landmarks tool of the program. After verification in the sagittal, coronal, and axial views, these landmarks were used to measure quantitative image variables ( Table I , Fig 1 ).
| Variable | Values and definition |
|---|---|
| Root resorption | Yes: surface defects >1 mm in length and depth No: no defects or defects ≤1 mm |
| Root resorption location | Apical third, middle third, cervical third, or combinations of regions, pulp involvement (yes/no) |
| Impacted canine (U3) development stages | Open apex Closed apex |
| Contact relationship with impacted canine | In contact: shortest distance between canine crown and adjacent root <1 mm Out of contact: shortest distance between canine crown and adjacent root ≥1 mm |
| Impacted canine crown mesiodistal position | Mesial: U3 cusp tip beyond lateral incisor (U2) mesial surface Middle: U3 cusp tip between U2 long axis and mesial surface Distal: U3 cusp tip distal to U2 long axis |
| Impacted canine crown buccal-palatal position | Buccal: U3 crown on the buccal side of adjacent teeth or near the buccal alveolar cortical plate Palatal: U3 crown on the palatal side of adjacent teeth or near the palatal alveolar cortical plate |
| Distance between impacted canine and target tooth long axis (mm) | Perpendicular distance from U3 cusp tip to the long axial plane of adjacent teeth |
| Angle between impacted canine and target tooth (°) | Superior-distal angle between U3 and adjacent tooth long axes |
| Distance between impacted canine and midsagittal plane (mm) | Perpendicular distance from U3 cusp tip to the midsagittal plane |
| Distance between impacted canine and occlusal plane (mm) | Perpendicular distance from U3 cusp tip to the occlusal plane |
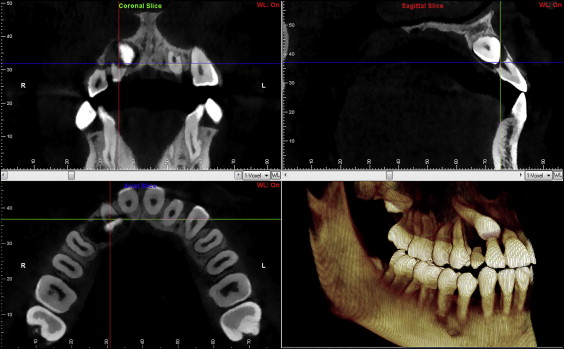
Categorical variables except for sex ( Table I ) were measured with both Mimics and Dolphin-3D (version 11.0; Dolphin imaging, Chatsworth, Calif) programs. The default segmentation ranges and the transparent mode in Dolphin-3D were used for its volumetric rendering. A positive finding of root resorption was assigned after its confirmation of both programs in the volumetric and 3 orthogonal views ( Fig 2 ).
To determine intrarater reliability, 40 patients were randomly chosen for a second analysis 1 month later.
Statistical analysis
Intrarater reliability was examined with the Cohen kappa (for categorical variables) and intraclass correlation tests (for quantitative variables).
The differences of root-resorption prevalence between the canine impaction and nonimpaction sides, between the impaction and control subjects, and between the buccal and palatal impactions were compared with chi-square tests. Resorption locations of root and pulpal involvement were assessed by descriptive statistics.
To identify risk factors for ICARR, all canine impaction sites (maxillary quadrants) were divided into 2 groups (with and without root resorption) for each affected tooth (central and lateral incisors, and first premolars). Chi-square (for categorical variables) and Wilcoxon (for quantitative variables) tests were used to compare the differences between the 2 groups for each variable. Wilcoxon tests instead of parametric tests were chosen because of the nonnormality of the data. Finally, step-wise forward logistic regressions were used, including those categorical and quantitative variables showing significance during the tests (chi-square or Wilcoxon) to identify the significant predicting factors for root resorption at each affected tooth.
Results
Overall, intrarater reliability for image assessment was excellent for both categorical (kappa tests, κ >0.9) and quantitative variables (intraclass correlations, r >0.9).
The prevalence rates of root resorption are shown in Tables II and III . Root resorption was significantly more prevalent in the canine-impaction subjects than in the controls ( Table II ). In subjects with unilateral canine impaction, root resorption was more prevalent at the impaction than the nonimpaction side ( Table III ). Despite a tendency for greater frequency of incisor root resorption in palatal impaction than in labial impaction in these subjects ( Tables II and III ), the differences were not statistically significant.
| Type of impaction | Central incisor | Lateral incisor | First premolar | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Impaction subjects | Control subjects | P † | Impaction subjects | Control subjects | P † | Impaction subjects | Control subjects | P † | |
| Buccal (n = 101/group) ∗ | 14.0% | 2.0% | 0.002 | 22.8% | 2.0% | <0.001 | 10.0% | 0.0% | <0.001 |
| Palatal (n = 69/group) ∗ | 23.2% | 4.3% | 0.001 | 34.3% | 2.9% | <0.001 | 8.7% | 0.0% | 0.012 |
| Combined (n = 170/group) ∗ | 17.8% | 2.9% | <0.001 | 27.4% | 2.4% | <0.001 | 9.5% | 0.0% | <0.001 |
∗ Sample size: subjects with missing target tooth (central incisor, 1 subject; lateral incisor, 2 subjects; first premolar, 1 subject) were excluded; a subject with bilateral impaction was treated as 1 sample (n = 1) for this analysis.
† Chi-square tests between impaction and control subjects for each target tooth; P <0.05 was considered statistically significant.
| Type of impaction | Central incisor | Lateral incisor | First premolar | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Impaction side | Normal side | P † | Impaction side | Normal side | P † | Impaction side | Normal side | P † | |
| Buccal (n = 93) ∗ | 12.0% | 0.0% | 0.001 | 21.5% | 0.0% | <0.001 | 10.9% | 0.0% | 0.001 |
| Palatal (n = 63) ∗ | 19.0% | 3.2% | 0.005 | 32.8% | 3.3% | <0.001 | 9.5% | 0.0% | 0.012 |
| Combined (n = 156) ∗ | 14.8% | 1.3% | <0.001 | 26.0% | 1.3% | <0.001 | 10.3% | 0.0% | <0.001 |
∗ Sample size of unilateral canine impaction subjects; subjects with missing target tooth (central incisor, 1 subject; lateral incisor, 2 subjects; first premolar, 1 subject) were excluded.
† Chi-square tests between the impaction and normal sides for each target tooth; P <0.05 was considered statistically significant.
ICARR was present predominantly at the apical third of all 3 teeth. The second most common location of ICARR was the middle third at the lateral incisor and the first premolar, and involving the entire root of the central incisor ( Table IV ). In addition, over 50% of ICARR reached the pulp at the central incisor, with only 36% at the lateral incisor and none at the first premolar ( Table IV ).
| Adjacent tooth | Apical 1/3 | Middle 1/3 | Cervical 1/3 | Apical-middle 2/3 | Involving entire root | Pulpal involvement |
|---|---|---|---|---|---|---|
| Central incisor (n = 35) ∗ | 37.1% | 8.6% | 2.9% | 17.1% | 34.3% | 57.1% |
| Lateral incisor (n = 47) ∗ | 44.7% | 27.7% | 8.5% | 4.3% | 14.9% | 36.2% |
| First premolar (n = 16) ∗ | 62.5% | 31.2% | 6.2% | 0.0% | 0.0% | 0.0% |
∗ Sample size with root resorption; a subject with bilateral impaction and resorption (central incisor, 5 subjects; lateral incisor, 1 subject; first premolar, 0 subject) was treated as 2 samples (n = 2) for the 2 impaction sites (maxillary quadrants).
Based on the analysis of each variable ( Table V ), contact relationship, mesiodistal position of the canine, distance between the impacted canine and the affected tooth, and distance between the impacted canine and midsagittal plane were factors that significantly affected the occurrence of ICARR at all 3 adjacent teeth. Canine development stage was a significant factor for ICARR at the incisors but not at the first premolar, whereas sex showed a significant effect on ICARR only at the central incisor.
| Variable | Adjacent central incisor | Adjacent lateral incisors | Adjacent first premolar | ||||||
|---|---|---|---|---|---|---|---|---|---|
| RR (–) ∗ | RR (+) ∗ | P † | RR (–) | RR (+) | P † | RR (–) | RR (+) | P † | |
| Categorical variables (number of impaction sites) ∗ | |||||||||
| Sex | 0.01 | 0.16 | 0.66 | ||||||
| Female | 75 | 26 | 70 | 30 | 93 | 8 | |||
| Male | 73 | 9 | 65 | 17 | 74 | 8 | |||
| Canine development stage | <0.01 | 0.01 | 0.38 | ||||||
| Open apices | 80 | 8 | 72 | 15 | 82 | 6 | |||
| Closed apices | 68 | 27 | 63 | 32 | 85 | 10 | |||
| Contact relationship | <0.01 | <0.01 | <0.01 | ||||||
| No contact | 112 | 8 | 34 | 1 | 130 | 6 | |||
| Contact | 36 | 27 | 101 | 46 | 37 | 10 | |||
| Bucco-palatal position | 0.16 | 0.08 | 0.77 | ||||||
| Buccal | 91 | 17 | 86 | 23 | 98 | 10 | |||
| Palatal | 57 | 18 | 49 | 24 | 69 | 6 | |||
| Mesiodistal position | <0.01 | <0.01 | <0.01 | ||||||
| Mesial | 37 | 27 | 41 | 21 | 64 | 0 | |||
| Middle | 38 | 4 | 25 | 18 | 39 | 4 | |||
| Distal | 73 | 4 | 69 | 8 | 64 | 12 | |||
| Quantitative variables (median) † | |||||||||
| Age (y) | 13.0 | 14.0 | 0.75 | 13.0 | 14.0 | 0.09 | 13.0 | 14.0 | 0.08 |
| Distance between impacted canine and target tooth long axis (mm) ‡ | 7.2 | 1.3 | <0.01 | 2.1 | −1.9 | <0.01 | 10.7 | 6.8 | 0.01 |
| Angle between impacted canine and target tooth (°) | 33.4 | 31.6 | 0.16 | 36.3 | 40.5 | 0.14 | 38.4 | 43.9 | 0.84 |
| Distance between impacted canine and midsagittal plane (mm) | 11.6 | 4.7 | <0.01 | 12.6 | 7.2 | <0.01 | 9.4 | 16.4 | <0.01 |
| Distance between impacted canine and occlusal plane (mm) | 8.9 | 9.7 | 0.26 | 8.9 | 9.4 | 0.84 | 9.1 | 10.4 | 0.71 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


