History of the Procedure
The American Heritage Medical Dictionary defines marsupialization as a surgical alteration of a cyst or similar enclosed cavity by making an incision and suturing the flaps to the adjacent tissue, creating a pouch. Various authors have described marsupialization, including Jacobson, who provided the first description in 1950 for management of the Bartholin duct cyst ( Figure 82-1 ). He constructed a mucocutaneous junction by suturing the cyst lining to the skin, thus creating a continuous decompression of the lesion. This was in contrast with drainage of the cystic lesion and packing the cavity with iodoform gauze, where failure occurred due to the retraction of wound edges and stenosis. With the introduction of various forms of catheters, the use of marsupialization seems to have declined. In oral and maxillofacial surgery, the use of marsupialization has been reported in the management of various odontogenic and nonodontogenic lesions such as the keratocystic odontogenic tumor and ranula.
History of the Procedure
The American Heritage Medical Dictionary defines marsupialization as a surgical alteration of a cyst or similar enclosed cavity by making an incision and suturing the flaps to the adjacent tissue, creating a pouch. Various authors have described marsupialization, including Jacobson, who provided the first description in 1950 for management of the Bartholin duct cyst ( Figure 82-1 ). He constructed a mucocutaneous junction by suturing the cyst lining to the skin, thus creating a continuous decompression of the lesion. This was in contrast with drainage of the cystic lesion and packing the cavity with iodoform gauze, where failure occurred due to the retraction of wound edges and stenosis. With the introduction of various forms of catheters, the use of marsupialization seems to have declined. In oral and maxillofacial surgery, the use of marsupialization has been reported in the management of various odontogenic and nonodontogenic lesions such as the keratocystic odontogenic tumor and ranula.
Indications for the Use of the Procedure
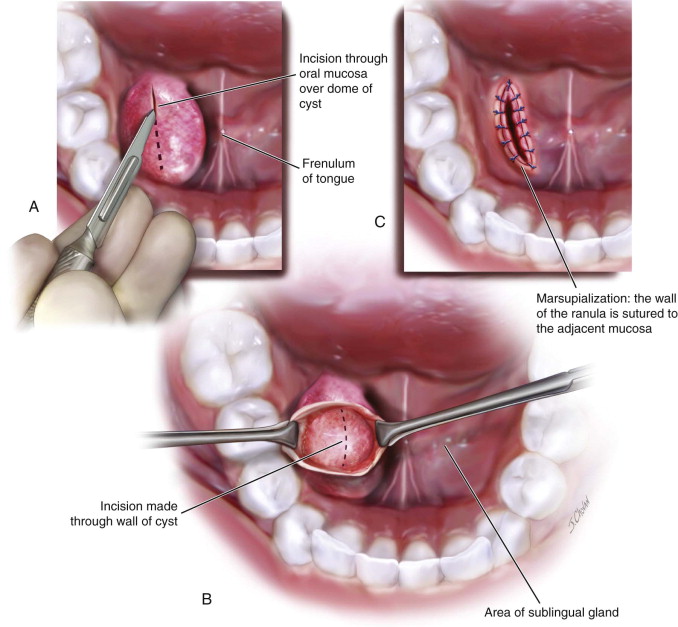
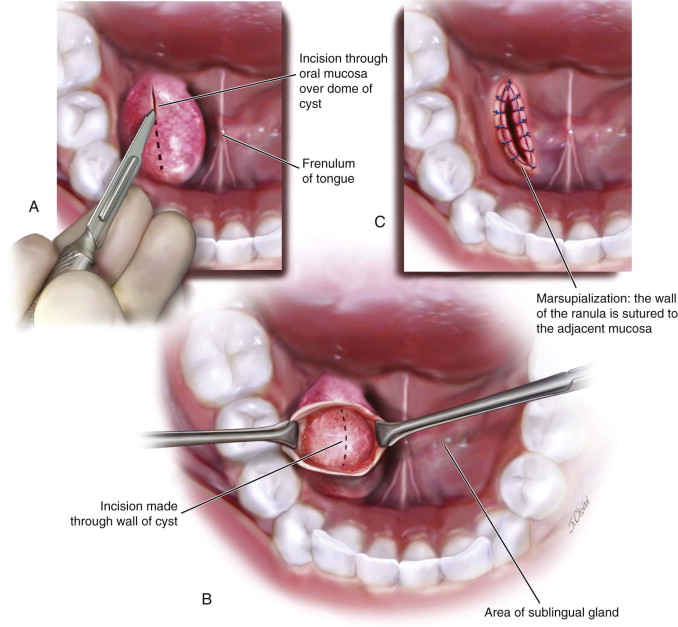
One indication for marsupialization is to create a new accessory tract for drainage of a gland. Various authors have reported this technique for the management of oral ranula, particularly in the pediatric population. However, the reported recurrence rate associated with simple marsupialization can range from 14% to 67%. Due to this recurrence rate, modification of the technique, including packing the marsupialized cavity, has been described. Based on a review of literature by Patel, the average rate of recurrence for oral ranula after simple or modified marsupialization is 20%. Excision of the ipsilateral sublingual gland along with the ranula has been demonstrated to be the most definitive treatment with the lowest rate of recurrence. However, despite its higher recurrence rate, marsupialization of oral ranula may be considered a first-line treatment.
Another indication is when continuous decompression of a lesion is desired, such as in the management of an odontogenic cyst. Marsupialization has been described as an effective treatment modality for the management of a keratocystic odontogenic tumor (KOT). Upon marsupialization and decompression, substantial histologic changes have been reported in the epithelium of a KOT. A treatment time of at least 9 months is required to demonstrate these histologic changes based on cytokeratin-10 immunohistochemical staining. These findings indicate that marsupialization can be an effective technique for managing a KOT. However, a recurrence rate of 12% has been reported with this technique. Despite these reports, marsupialization is an effective treatment modality for managing a KOT.
Marsupialization has been reported in the management of benign odontogenic tumors such as ameloblastoma. However, the rate of recurrence continues to be concerning.
Limitations and Contraindications
Use of marsupialization is limited to cystic lesions that require continuous drainage and therefore cannot be utilized to manage solid lesions. The utility of marsupialization is debatable when the lesion is not composed of an epithelial lining that can be sutured to the surrounding mucosa or skin. Marsupialization is contraindicated when previous attempts at conservative treatment have failed and when complete or marginal resection is indicated.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


