The proper eruption and final position of the canine tooth is an essential part of the maturation of the dentition to ensure proper occlusion and optimize the esthetic appearance of the patient’s smile. Abnormal eruption or failure of the eruption of the canine can result in malposition and periodontal compromise of adjacent teeth, loss of arch space, internal or external resorption of the canine or adjacent teeth, formation of cysts associated with the impacted tooth, and recurrent infection with a partially erupted canine. Impacted canines complicate orthodontic treatment, potentially compromising the occlusion and esthetic outcome of the case. Early diagnosis, surgical and orthodontic manipulation to prevent impaction and to manage the impacted teeth, is essential in obtaining an optimal outcome for the patient.
Etiopathogenesis/Causative Factors
The maxillary canines are the second most frequently impacted teeth after wisdom teeth, with incidence reports in the literature in the range of 1% to 3.5% in the general population. Mandibular canine impaction occurs at a much lower rate, possibly about 0.3%. These rates would be much higher in a cohort of patients undergoing orthodontic treatment. Peck et al, in a review of the literature on palatally impacted canines, reports the incidence of bilateral maxillary canine impaction at 17% to 45%. The rate among female patients is twice as high as among males: 1.17% versus 0.51%.
The anomaly of canine impaction has been attributed to genetic and local factors. Although the actual cause is probably multifactorial, genetic and guidance theories of causation have been proposed. Proponents of the genetic theory—the assumption that the impaction is under genetic influence—identify increased occurrence of other dental anomalies, bilateral occurrence of impaction, familial occurrence, sex differences, and population differences as support for the genetic theory of impaction. The guidance theory is based on more local factors influencing the proper eruption of the canine. Some authors have used the same data proposed by Peck et al to support their guidance theory of impaction. Bishara identified multiple factors that are likely involved in the etiology of the impacted canine: (1) tooth size–arch length discrepancies, (2) prolonged retention or early loss of the deciduous canine, (3) abnormal position of the tooth bud, (4) the presence of an alveolar cleft, (5) ankylosis, (6) cystic or neoplastic formation, (7) dilacerations of the root, (8) iatrogenic, (9) trauma, and (10) idiopathic, including primary failure of eruption. In most cases, it is difficult to identify the precise etiologic factor leading to the impaction of the canine.
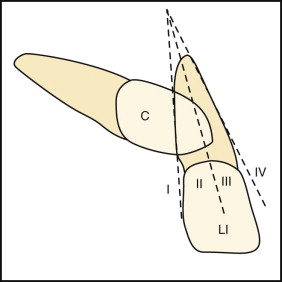
Prediction of canine impaction in the maxilla has been evaluated by multiple authors. Warford et al evaluated the prediction of maxillary canine impaction after primary canine extraction in patients less than age 12 years using sector localization and angular measurements based on panographic radiographs. The location of the cusp tip of the canine in question and its relationship to the adjacent lateral incisor was divided into specific sectors: Sector I represents the area distal to a line tangent to the distal heights of contour of lateral incisor crown and root; sector II is mesial to sector I, but distal to the bisector of the lateral incisor’s long axis; sector III is mesial to sector II, but distal to the mesial heights of contour of the lateral incisor crown and root; and sector IV includes all areas mesial to sector III ( Fig. 16-1 ). The findings in Warford’s study indicate that of the two factors considered for predicting maxillary canine impaction, canine angulation and sector location, the prediction appears to rest almost solely on the sector location of the cusp tip of the erupting canine. As shown by the predictive values for sector location alone—(I) 0.06, (II) 0.38, (III) 0.87, and (IV) 0.99—the more mesial the cusp tip location, the greater the likelihood of impaction. The overall incidence of impaction was 82%, if the canine cusp tip was in sections II, III, or IV. In any patient where the tip of the canine overlaps the root of the lateral incisor in a Panorex film, orthodontic evaluation and possible early intervention would be appropriate.
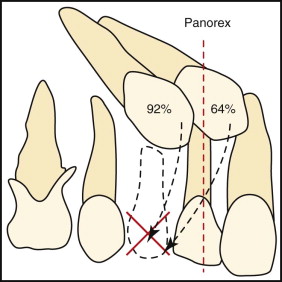
Ericson also showed that the position of the crown of the canine in relationship to the root of the lateral incisor is a key determinant in the potential for eruption or impaction of the maxillary canine after primary canine extraction. If the crown of the canine was distal to the midline of the lateral incisor root, the canine erupted 92% of the time, whereas if it was mesial to the midline of the root, eruption occurred in 64% of the cases after primary canine extraction ( Fig. 16-2 ).
Diagnostic Studies
Early detection of the potential for canine impaction is important, because early intervention can reduce the treatment time, complexity, and complications. The earliest and most simple method for early detection involves visual inspection and tactile clinical examination by the age of 9 to 10 years. The maxillary and mandibular canine usually erupts around age 10 to 12 years, with a buccal bulge usually palpable at least 1 year before eruption. The diagnosis of an impacted maxillary canine is done using both clinical examination and radiographic assessment ( Fig. 16-3 ). Clinical signs that might indicate canine impaction include over-retained or asymmetry in exfoliation of the primary canine, lack of canine bulge on the buccal aspect of the ridge by age 10 years, asymmetry of the buccal canine bulge, palatal bulge in the canine region, lack of deciduous canine root resorption, and malposition of the adjacent lateral incisor.
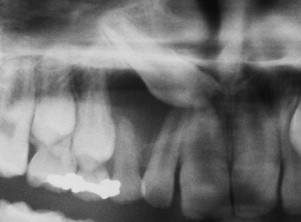

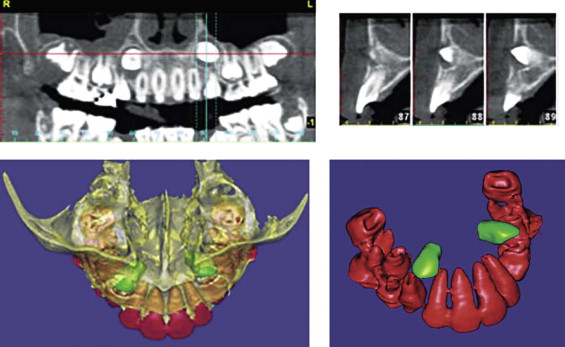
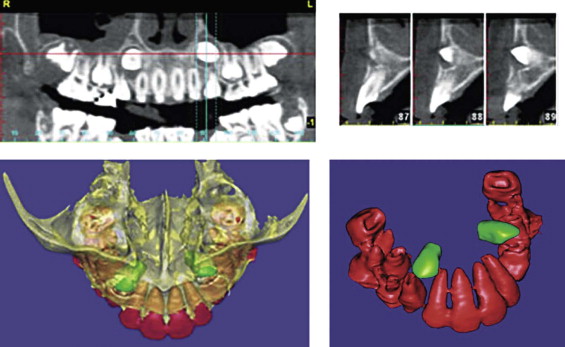
Radiographs useful for diagnosis and evaluation of impacted canines include panographic, periapical, occlusal, and lateral cephalometric plain films. Using Clark’s rule, plain films can usually assist in the determination of the relative buccal-lingual position of the impacted tooth, that is, if the object moves the same direction as the movement of the beam, then it is on the buccal aspect of the ridge; if movement is in the opposite direction, then it is on the lingual aspect of the ridge. Cone beam CT scanning, with or without three-dimensional (3D) reconstruction, provides an opportunity for exact localization of the impacted canine. Walker et al showed the benefits of 3D volumetric imaging of impacted canines, which can demonstrate presence or absence of the canine, size of the follicle, inclination of the long axis of the tooth, relative buccal and palatal positions, amount of the bone covering the tooth, 3D proximity and resorption of roots of adjacent teeth, condition of adjacent teeth, local anatomic considerations, and overall stage of dental development, root form, and the presence of pathology or adverse conditions affecting the impacted tooth. This information assists the orthodontist in planning the mechanics that will be used to guide the eruption of the tooth while minimizing the risks to the adjacent teeth ( Fig. 16-4 ).
Most references note the preponderance of maxillary canine impaction on the palatal (85%) versus buccal (15%) aspect of the ridge. These data have been based on plain film evaluation and primarily on the mode of surgical access to the impacted maxillary canines. Recent evaluation of the canine position by Liu et al, using cone beam CT scanning to definitively determine the position of the impacted maxillary canine results, showed a different distribution: 45.2% impacted buccally, 40.5% impacted palatally, and 14.5% impacted midalveolus. The majority of maxillary canine impactions are, in fact, most easily approached from the palatal aspect of the ridge, but exact localization to determine the best surgical approach is of paramount importance. The cone beam CT technology allows the precise localization of the impacted tooth.
Diagnostic Studies
Early detection of the potential for canine impaction is important, because early intervention can reduce the treatment time, complexity, and complications. The earliest and most simple method for early detection involves visual inspection and tactile clinical examination by the age of 9 to 10 years. The maxillary and mandibular canine usually erupts around age 10 to 12 years, with a buccal bulge usually palpable at least 1 year before eruption. The diagnosis of an impacted maxillary canine is done using both clinical examination and radiographic assessment ( Fig. 16-3 ). Clinical signs that might indicate canine impaction include over-retained or asymmetry in exfoliation of the primary canine, lack of canine bulge on the buccal aspect of the ridge by age 10 years, asymmetry of the buccal canine bulge, palatal bulge in the canine region, lack of deciduous canine root resorption, and malposition of the adjacent lateral incisor.


Radiographs useful for diagnosis and evaluation of impacted canines include panographic, periapical, occlusal, and lateral cephalometric plain films. Using Clark’s rule, plain films can usually assist in the determination of the relative buccal-lingual position of the impacted tooth, that is, if the object moves the same direction as the movement of the beam, then it is on the buccal aspect of the ridge; if movement is in the opposite direction, then it is on the lingual aspect of the ridge. Cone beam CT scanning, with or without three-dimensional (3D) reconstruction, provides an opportunity for exact localization of the impacted canine. Walker et al showed the benefits of 3D volumetric imaging of impacted canines, which can demonstrate presence or absence of the canine, size of the follicle, inclination of the long axis of the tooth, relative buccal and palatal positions, amount of the bone covering the tooth, 3D proximity and resorption of roots of adjacent teeth, condition of adjacent teeth, local anatomic considerations, and overall stage of dental development, root form, and the presence of pathology or adverse conditions affecting the impacted tooth. This information assists the orthodontist in planning the mechanics that will be used to guide the eruption of the tooth while minimizing the risks to the adjacent teeth ( Fig. 16-4 ).
Most references note the preponderance of maxillary canine impaction on the palatal (85%) versus buccal (15%) aspect of the ridge. These data have been based on plain film evaluation and primarily on the mode of surgical access to the impacted maxillary canines. Recent evaluation of the canine position by Liu et al, using cone beam CT scanning to definitively determine the position of the impacted maxillary canine results, showed a different distribution: 45.2% impacted buccally, 40.5% impacted palatally, and 14.5% impacted midalveolus. The majority of maxillary canine impactions are, in fact, most easily approached from the palatal aspect of the ridge, but exact localization to determine the best surgical approach is of paramount importance. The cone beam CT technology allows the precise localization of the impacted tooth.
Treatment Goals/Options
The treatment goals for management of the impacted canine include:
- •
Eruption of the impacted canine into the arch with functional occlusion
- •
Maintenance of an adequate zone of attached tissue on the buccal and lingual aspects of the canine as it is erupted into the mouth
- •
Esthetic gingival contours once the impacted canine is in position
- •
Minimizing or avoiding damage to the adjacent teeth, maintaining an intact periodontium
Several factors must be taken into consideration in determining the treatment option chosen for management of the impacted canine, including:
- •
Patient age
- •
General dental health and oral hygiene
- •
Whether space is available within the arch or if it can be established with orthodontic manipulation
- •
Suitability of the first bicuspid to replace the canine
- •
Favorability of the position of the impacted canine and the likelihood of being able to get it into position with orthodontic treatment
- •
Patient motivation for orthodontic treatment
- •
Medical contraindications for surgery
Pitt et al asked orthodontists to evaluate several factors that will influence the difficulty of treatment in order to develop a “treatment difficulty index” with which to preoperatively evaluate impacted canine cases. Their analysis showed that the horizontal position, as measured by the degree of overlap of the lateral and central incisors by the crown of the impacted canine, is the most important factor in determining the difficulty of aligning the unerupted tooth. Patient age was the next most important factor, followed by vertical height and buccopalatal position. Becker and Chaushu evaluated the effects of age on success of orthodontically erupting impacted canines by looking at 38 matched cases in a series of adults (mean age 29.8 ± 8.6) versus young patients (mean age 13.7 ± 1.3). They found 100% success in the young patients and 69.5% in the adults, with all of the failures being in patients older than age 30 years.
Multiple treatment options are available to manage impacted canines; the treatment is chosen after consultation between the surgical team and treating orthodontist:
- •
Retention of the impacted canine in place with serial radiographic observation to check for development of asymptomatic pathosis with or without retention of the primary canine
- •
Extraction of the impacted tooth and retention of the primary canine with restorative procedures to improve its esthetic contours
- •
Extraction of the impacted tooth and primary canine followed by orthodontic space closure, substituting the first bicuspid for the extracted canine (“bicuspid substitution”)
- •
Extraction of the impacted tooth and primary canine with replacement using an implant-supported crown
- •
Surgical exposure of the impacted canine with orthodontic alignment of the ectopic tooth after its surgical exposure
- •
Autotransplantation of the impacted tooth into its anatomic position in the arch after orthodontic pretreatment for space opening
Surgical Management of Impacted Canines
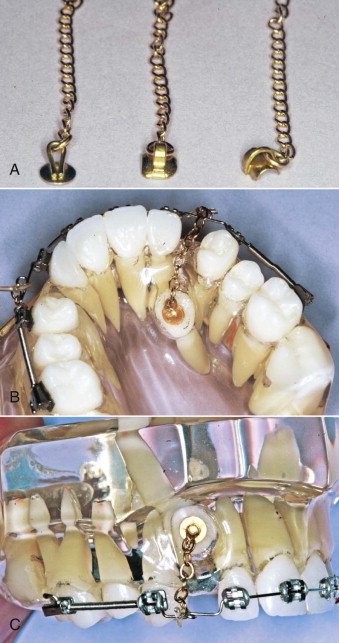
Most of the literature available today is related to the impaction of maxillary canines, reflecting their 20-fold greater occurrence than impacted mandibular canines. The typical management involves orthodontic manipulation to provide adequate space for the tooth in the arch and surgical access to the impacted tooth, with bonding of an orthodontic eruption device consisting of an orthodontic bracket/gold chain combination to the crown of the tooth ( Fig. 16-5 ).
Armamentarium for Exposure/Bonding Procedure
Instruments and supplies needed for the surgical procedure of exposing and bonding an eruption device to an impacted canine include:
- 1
Surgical instrumentation to allow incision, flap reflection, and suturing of the soft tissue as required
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


