Introduction
The purpose of this study was to identify variables of dental malocclusion with the greatest effect on sound production that can be easily identified during an orthodontic assessment.
Methods
One hundred fifteen patients (8.2-36 years of age) seeking orthodontic evaluation were assessed for speech sound production abnormalities. An orthodontic clinical examination assessed Angle classification, overjet, overbite, crowding, spacing, and crossbites. A standard speech sample was elicited from each subject.
Results
The results indicated that 71 (62%) of the subjects made a production error, particularly with the /s/ and /t/ sounds. However, auditory distortions occurred in 12 subjects (20%), and 56 (80%) subjects had visual distortions of the sound. An open bite (>2 mm) was the key malocclusal factor underlying speech sound errors. There was statistical significance between the Orthodontic Treatment Priority Index and the sound errors of /s / and /t/ (mean score of 9.54 vs 6.29 for subjects without sound errors).
Conclusions
Predictive malocclusal traits are associated with speech sound production errors. The more severe or handicapping the malocclusion, the more likely that a speech sound error will occur. Open bites of 2 mm are associated with sound production errors. Visual inaccuracy of the sound occurs with more frequency than auditory inaccuracy and is the most common articulation error noted with occlusal irregularities.
Highlights
- •
We compared occlusal features to speech samples in 115 subjects, 8 to 36 years old.
- •
Predictable malocclusal traits were associated with speech sound errors.
- •
The more handicapping the occlusion, the more likely the speech errors.
- •
Open bite was the feature most associated with sound distortions, especially /s/ and /t/.
- •
Lingual protrusion (lisp and tongue thrust) was the typical visual inaccuracy.
Traditionally, orthodontic care focuses primarily on dental esthetics and masticatory function. However, the clinician can often overlook the impact of malaligned teeth and skeletal arches on sound production. Since normal sound production and the oral cavity interact in a dynamic relationship, the orthodontist should possess the ability to recognize and determine how dental anomalies and orthodontic treatment relate to sound production. This provides enhanced patient care through improved treatment planning and appropriate referrals to speech pathologists for patients whose malocclusion impacts speech sound production. As clinicians, we need to be aware of any potential effects of malocclusion on speech sound production. This has become increasingly important as orthodontic practices continue to render more care to adults who require proper speech as part of their profession.
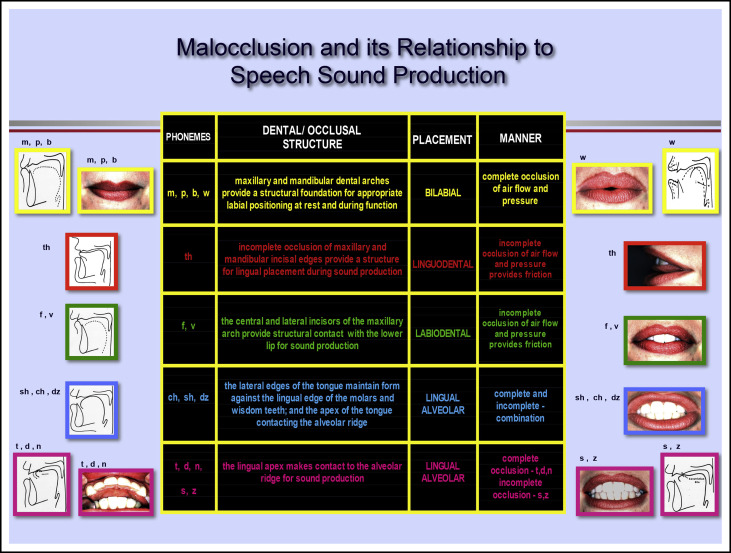
The dental arches (dentition and skeletal arch), acting as structural boundaries for placement of the tongue and lips, are inherently involved in the production of sounds for meaningful communication ( Fig ). Nearly 90% of all consonants are made in the anterior portion of the oral cavity, suggesting that the dental arch relationship may be one of the most important factors affecting articulation. A deviation in dental structure or alignment may interfere with the normal process of air flow and pressure, as well as proper lip and tongue placement and contouring, thereby affecting the integrity of speech sound production. The speech pathology and dental literature historically has had an interest in the impact of the dentition on speech. Studies have demonstrated the use of different articulatory postures to functionally adapt to variations in structural anomalies of the dental-skeletal framework and dentition, including occlusal plane, palatal shape, lingual shape and placement, and dentition.
Much research has resulted in findings that are often difficult for the dental specialist to detect in a routine orthodontic assessment. Acoustic changes such as variations in vowel production have been noted in persons with Class II and Class III malocclusions due to adaptive changes in tongue placement and contouring ; changes in mandibular movement caused by increased overjet ; changes in the production of /s/ affecting amplitude, velocity, and duration of placement and manner ; and changes in lip position, incisor, and tongue position, which depend on what was being said: ie, the complexity and the context. Although these findings are relative to the study of the pathophysiology of sound production and dental malocclusion, they provide little assistance in specifically addressing the risk factors, type of presentation, and specific information for counseling persons seeking orthodontic care on the effects of malocclusion on speech sound production.
The 3 dental or occlusal anomalies classically noted to have a negative impact on sound production are open bite, mandibular prognathism, and mandibular retrognathism. These studies have typically focused on small sample populations, patients with severe dental abnormalities, and single occlusal traits, such as Angle classification. Few authors have comprehensively studied multiple occlusal variables, indexes, and basic fundamental physiologic speech sound changes available to the dental specialist, namely, whether the perceived sound error is actually an error of auditory distortion of the sound or is a visual distortion only. In a visual distortion, the properties of the targeted sound are retained (the sound has normal acoustic properties to the listener’s ear), although lingual protrusion may be seen. The purpose of this study was to determine the effects, if any, of malocclusion on sound production by using auditory and visual descriptions to explain the relationships between various occlusal anomalies and sound production. Our hypothesis was that occlusal anomalies do not create any auditory or visual changes to the production of sounds.
Material and methods
Once internal review board approval was received at Montefiroe Medical Center, all persons coming to the Department of Dentistry, Division of Orthodontics over a 4.5-month period seeking orthodontic consultation before any active treatment were asked to take part in this study. One hundred fifteen patients agreed to participate in the investigation by signing the consent document. The subject pool comprised 50 male (43%) and 65 female (57%) patients ranging from 8 years 2 months to 36 years in age (mean, 12 years 10 months). Eight years of age was selected as the minimal age criterion because oral motor structure and function and normal speech sound production are considered to be mature (at the adult stage) and well integrated at this age. This age distribution represented a cross section of patients typically seen in an orthodontic practice.
The subjects signed the consent. A questionnaire was used to exclude patients with anatomic and physiologic disabilities such as mental retardation, neurologic disorders, overt dysmorphology (eg, cleft lip and palate, hypertrophic adenoids or tonsils), thumb sucking or other oral habits, retained infantile swallowing pattern, thrusting of the tongue (compared with an anterior lingual position) during speaking or swallowing, ankyloglossia, presence or history of previously diagnosed speech disorder and hearing deficits, and previous speech therapy or orthodontic care.
The subjects were primarily of Hispanic ethnicity and lived in nearby areas. Speaking another language, in addition to English, as the primary spoken language was not an exclusionary criterion in our sample (32% spoke Spanish as the primary language at home). Although there are linguistic differences between English and Spanish, these dissimilarities were not confounding to the parameters in this study.
After we received consent, we performed a thorough orthodontic evaluation and obtained and recorded a speech sound sample as outlined below.
A chairside orthodontic examination was conducted by the principal investigator (K.M.L.) to assess the following dental characteristics and variables: (1) Angle classification, (2) overjet, (3) overbite (open bite), (4) anterior crossbite, (5) posterior crossbite (unilateral or bilateral), (6) maxillary crowding, (7) mandibular crowding, (8) maxillary spacing, and (9) mandibular spacing.
Any rotated or displaced teeth and missing incisors along with the number of teeth in crossbite were also noted for calculation of the Orthodontic Treatment Priority Index (OTPI) of Grainger for each subject, thereby permitting an objective ranking of the subjects according to the severity of their malocclusions (degree of handicapping or priority for treatment). In addition, the index identified groups of malocclusal traits that occurred jointly and were called “syndromes” (case types).
The speech sample was obtained in a video imaging room in the Department of Dentistry to eliminate any ambient noise. Each subject was seated in an upright position with a mounted video camera recorder (Hi8 Handycam, model CCD-TR700; Sony, Tokyo, Japan) 12 to 18 inches from his or her face. The camera’s image was viewed on the monitor of a Macintosh computer (Apple, Cupertino, Calif) linked to the video recorder for imaging purposes. Each image incorporated the subject’s mouth and perioral structures, extending from the base of the nose to the bottom of the chin. Zoom capabilities facilitated careful inspection of the details of labial and lingual movement during sound production.
To enhance the acoustic proficiency of the video recorder, each subject held an omni-directional microphone (F-V5 dynamic microphone; Sony) at shoulder height, approximately 2 inches below chin level. The microphone’s cord fed directly into the audio input socket of the video recorder.
Speech sound productions were made via a verbal imitative task. During this process, the investigator could not be seen by the subject to eliminate any possible bias of using a visual model for the speech sample. The subjects were asked to repeat a standard speech sample of syllables, words, and phrases. Each audio-recorded speech sample was transcribed according to International Phonetic Alphabet standards. Judgments on lingual and labial movements during sound production were made on the video recordings.
The target sounds examined were /m/, /p/, /t/, /f/, /s/, /sh/, /ch/, /th/, and /l/. These consonants were chosen because their physiologic and distinctive properties are the same in Spanish and English and are determined in part by the structures in the anterior oral cavity (maxilla, mandible, tongue, teeth, and alveolar ridge). The target sounds were voiceless, produced with no vibration of the vocal folds, with the exception of /m/ and /l/. Sounds /z/, /d/, /v/, and /b/ were not included as variables in this study because they represented the same manner and placement as their respective counterparts /s/, /t/, /f/, and /p/, yet have increased laryngeal movement (voicing) during speech sound production. In addition, voicing as a parameter was excluded from this study to minimize the linguistic differences between Spanish and English, For example, /s/ and /z/ in English are 2 different phonemes (sounds), both appearing in written words in English and Spanish; however, the typical pronunciation for /z/ is /s/ in Spanish (with some dialect differences).
The investigation entailed a distinctive feature analysis of sound production of each of the target sounds at the isolated sound, syllable, word, phrase, counting, and conversation level. The speech sound variables included (1) the target sounds /m/, /p/, /t/, /f/, /s/, /sh/, /ch/, /th/, and /l/; (2) any placement errors; (3) the severity of the sound error; and (4) the type of distortion (visual inaccuracy, articulatory [auditory] distortion, or a combination of them).
Placement errors were characterized by anterior lingual protrusion (extension of the lingual apex at least 2 mm beyond the maxillary or mandibular incisal edges during an attempted sound), dental edge contact (the lingual apex making contact with the maxillary or mandibular incisal edges but not more than 1 mm beyond the edge during an attempted sound), lip excursion (the lower lip abnormally extending to the upper lip for production of the interdental sound /f/, as with severe prognathism or lip incompetence), lingual retraction (retraction of the tongue in a posterior or superior position in the oral cavity for production of the linguoalveolar /s/, /l/, or /sh/, as with a severe open bite), and lateral lingual protrusion (the tongue protrudes through a lateral open bite during production of /t/, /s/, and /sh/).
Statistical analysis
For categorical variables, the associations between Angle classification, anterior crossbite, posterior crossbite, and presence or absence of each type of sound production variable (target sound, error, distortion) were tested for significance using the chi-square test. For the continuous variables, such as maxillary and mandibular crowding and spacing, the association with the sound production variable was tested for significance with Pearson correlation coefficients. Since the Grainger scale was ordinal, the association with each sound production variable was tested for significance using the Wilcoxon rank sum test. Relative frequency distributions were calculated for each type of sound production variable, as well as for categorical dental malocclusion variables. Means and standard deviations or medians and ranges were calculated for each continuous variable as appropriate. All tests of significance were 2 tailed and performed using a type I error of .05.
For the orthodontic reliability, 1 investigator (K.M.L.) was responsible for the orthodontic measurements that were assessed and recorded. Intrajudge reliability was determined by having the investigator obtain measurements directly from the subject during a clinical examination and then from dental models of the subject later. This was done for 25 subjects and showed a reliability of 94%.
For the speech reliability, a panel of 1 speech physiologist (E.M.L.) and 2 speech pathologists served as evaluators of the speech sound samples. The panel demonstrated an interjudge reliability of 86%.
Results
The orthodontic clinical examination showed that 60 (52%) subjects had an Angle Class I malocclusion, 47 (41%) had a Class II malocclusion (Division 1, 43; Division 2, 4), and 8 (7%) had a Class III malocclusion. Although all 115 subjects had some degree of malocclusion, 44 subjects (38%) showed normal sound production with equal frequency across all occlusal traits, with an open bite of 2 mm or less.
Seventy-one subjects (62%) demonstrated a sound production error. The number of subjects with a production error differed for each of the 9 target sounds. No differences were noted across age distributions. The sounds were divided into 5 groups depending on their cluster of presentation:
Group 1: No sound production errors, n = 44 (38%).
Group 2: Sound production errors with /s/, n = 14 (12%).
Group 3: Sound production errors with /t/, n = 8 (7%).
Group 4: Sound production errors with /s/ and /t/, n = 41 (36%).
Group 5; Sound production errors with any or a combination of /m/, /p/, /f/, /th/, /sh/, /ch/, or /l/, n = 8 (7%).
Production errors were assessed with regard to inappropriate lip and tongue placement during sound production. Observations were made on whether the placement errors resulted in visual inaccuracies (normal acoustic properties with visual distortion), articulatory distortions (abnormal acoustic properties, auditorily incorrect), or a combination of the two. Placement errors were noted in all types of sounds produced by the 71 subjects who had a production error. However, auditory distortions occurred in 12 subjects (20%; 2 subjects had auditory distortions, and 12 subjects had a combination of auditory and visual distortions), and 56 (80%) subjects had a visual distortions of the sound.
Visual inaccuracies occurred in 56 (79%) of the 71 subjects who demonstrated a production error. Lingual protrusion and dental edge contact accounted for 60% of all placement errors. Lingual protrusion was by far the most common placement error. All of the 14 subjects (100%) who misarticulated /s/ exhibited only lingual protrusion. Visual inaccuracies were noted, with the most frequency with the /s/ sound, whether it occurred in isolation (no other errors) or concurrently with /t/. Thirty-nine (95%) of the 41 subjects with a production error for /s/and /t/ exhibited lingual protrusion. Of the 8 subjects who misarticulated /t/, only 5 (63%) had dental edge contact; the remaining 3 subjects (37%) had lingual protrusion. Visual inaccuracies were highly correlated with the placement error of lingual protrusion. Articulatory distortions occurred with less frequency in 14 (20%) of the 71 subjects who had a production error. This distortion type caused the target sound to be produced inaccurately and perceived as such by the listener. Articulatory distortions occurred with the greatest frequency with the /s/ sound.
The associations between the variables of malocclusion and the OTPI of Grainger and each sound production variable were assessed for significance using chi-square tests. Interestingly, there was no significant relationship between any speech sound variable and Angle classification, overjet, overbite (not including open bites), anterior crossbite, maxillary crowding or spacing, and mandibular crowding or spacing. However, significant trends did occur with the speech variables and the malocclusion traits, such as open bite and posterior crossbite.
The OTPI values ( Table I ) were significantly higher in subjects with production errors. The mean value was 9.54 for those who demonstrated placement errors for the /s/ and /t/ sounds, particularly lingual protrusion, compared with 6.29 for subjects without placement errors. Similarly, the mean value was 9.01 for subjects who had a visual inaccuracy, compared with 6.25 for those who did not.
| n | Mean OTPI | SD | Range | |
|---|---|---|---|---|
| Normal articulation | 44 | 6.35 | 4.63 | 0.27-18.27 |
| /s/ errors | 14 | 7.04 | 4.83 | 0.57-15.87 |
| /t/ errors | 8 | 5.78 | 2.90 | 0.67-8.60 |
| /s and t/ errors | 41 | 10.94 ∗ | 6.08 | 1.37-26.02 |
| Other sound errors | 8 | 4.88 | 4.23 | 0.67-12.92 |
| No placement errors | 57 | 6.29 | 4.56 | 0.27-18.27 |
| Placement errors | 58 | 9.54 † | 5.96 | 0.67-26.02 |
| No distortions | 45 | 6.25 | 4.63 | 0.27-18.27 |
| Distortions | 71 | 9.01 ‡ | 5.83 | 0.57-26.02 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


