Introduction
The flexible spiral wire (FSW) canine-to-canine lingual retainer bonded to all 6 anterior teeth is a frequently used type of mandibular fixed retainer. This study aimed to assess the long-term effectiveness of FSW canine-to-canine lingual retainers in maintaining the alignment of the mandibular anterior teeth after orthodontic treatment.
Methods
The sample consisted of dental casts of 221 consecutively treated patients (75 girls, 146 boys) from the archives of the Department of Orthodontics and Craniofacial Biology, Radboud University Nijmegen Medical Center, The Netherlands, who received a FSW canine-to-canine lingual retainer bonded to all 6 anterior teeth after active orthodontic treatment. The casts were studied before treatment (Ts), immediately after treatment (T0), 2 years (T2), and 5 years (T5) posttreatment.
Results
The main irregularity index decreased significantly from 5.40 mm (SD, 3.47) at Ts to 0.07 mm (SD, 0.23) at T0. At T5, the alignment of the mandibular anterior teeth was stable in 200 patients (90.5%); in 21 patients (9.5%), a mean increase of 0.81 mm (SD, 0.47) was observed. The increase of irregularity was strongly related to the bonding failures of the retainer. In 6 patients (2.7%), unexpected posttreatment complications (torque differences of the incisors, increased buccal canine inclination) were observed.
Conclusions
The FSW canine-to-canine lingual retainer is very effective in maintaining the alignment of the mandibular anterior region after active orthodontic treatment. However, regular checkups are necessary to determine bonding failures, posttreatment changes, and complications as early as possible.
Many studies have demonstrated a high relapse rate of the alignment of the mandibular anterior teeth after orthodontic treatment and retention. From the various types of removable or fixed mandibular retainers used to prevent relapse in the mandibular arch, the flexible spiral wire (FSW) canine-to-canine retainer bonded to the lingual surfaces of all 6 mandibular teeth is commonly used. Although these retainers are widely used, only a limited number of studies deal with their long-term effectiveness. Littlewood et al found in their Cochrane review only 1 prospective randomized clinical trial that assessed the stability of incisor alignment after 3 years of retention. One of the 4 test groups in this study received retainers bonded to all 6 anterior teeth (n = 11) and experienced no increase in incisor irregularity (in the 8 patients with no detachment of the retainer). Similar results were reported in a prospective study that was excluded from the Cochrane review. This study compared a small group of patients (n = 34) who received mandibular retainers bonded only to the canines with 2 groups of patients (n = 31 and 38) who received 2 types of retainers attached to all anterior teeth. After an observation period of 2 years, no relapse was observed in patients with a 0.0195-in FSW canine-to-canine retainer, whereas the relapse rate in patients with a 0.0215-in FSW canine-to-canine retainer was 20%. However, in both FSW groups, the changes in the irregularity index were not significant.
In a recent retrospective study, a 0.65-mm mean increase in the irregularity index was shown 1 year after treatment in a small group of patients (n = 29) retained with FSW retainers. This increase was not significantly different when compared with a group of 29 patients who received a removable retainer.
The shortcomings of the available literature (small patient groups or short observation periods) considerably restrict the evidence about the stability of orthodontic alignment of the mandibular anterior teeth retained with the FSW canine-to-canine lingual retainer. Therefore, we aimed to assess the long-term effectiveness of mandibular FSW canine-to-canine retainers bonded to all 6 teeth in a large consecutive group of patients.
Material and methods
Our material consisted of dental casts from the archives of the Department of Orthodontics and Craniofacial Biology, Radboud University Nijmegen Medical Center, The Netherlands. We selected 221 patients who were treated with full fixed appliances and received a mandibular lingual FSW retainer (0.0195-in, 3-strand, heat-treated twist wire, Wildcat, GAC International, Bohemia, NY), bonded to all 6 mandibular anterior teeth at the end of active orthodontic treatment ( Fig 1 ). Dental casts and intraoral photographs were available before treatment (Ts), after treatment (T0), at least 2 years after treatment (T2), and at least 5 years after treatment (T5). Patients with spacing or missing teeth in the mandibular anterior region before or after treatment and retreated patients with any orthodontic appliance were excluded.

No interproximal enamel reduction or circumferential supracrestal fiberotomy was systematically performed.
The measurements for both the intercanine distance and the irregularity index were made with an electronic caliper (digital 6, Mauser, Winterthur, Switzerland) with an accuracy of 0.01 mm. The beaks of the electronic caliper were sharpened to a fine edge to permit access and make accurate measurements.
The intercanine distance was measured from the middle of the cusp of the mandibular left canine to the middle of the cusp of the mandibular right canine. In case of abrasion of a cusp, an estimation of the middle of the surface was made.
The irregularity index ( Fig 2 ) was used to describe the contact point displacement of the mandibular anterior teeth. The irregularity index is the sum (in millimeters) of the 5 distances between the anatomic contact areas from the mesial aspect of the left canine through the mesial aspect of the right canine. When anatomic contact points of adjacent teeth are touching, the measurement is zero. With increased irregularity, greater displacement led to an increased index score. Before measurement, the anatomic contact areas of the mandibular incisors and the mesial anatomic contact areas of the canines were marked on the dental casts. The linear distance between the markings was then measured, and the 5 values were added. Because the beaks of the caliper were sharpened, it was possible to measure small distances. The measurements were made at Ts, T0, T2, and T5. At T0, T2, and T5, the measurements were rounded to 0.25, 0.50, and 0.75 mm. Patients with scores less than 0.25 mm were considered as having a perfect irregularity index.

Sex, age, treatment duration, and failures were obtained from the patient files. Angle classification was determined on the right side of the plaster models. Sagittal contact of the incisors after treatment was determined from the plaster models in occlusion. Regarding extractions, the patients were divided into 4 categories: (1) nonextraction, (2) extraction of 1 premolar in every quadrant, (3) no extraction in the mandibular arch and extraction of 1 premolar or first molar in both maxillary quadrants, and (4) a rest group (extraction of the second molars, unilateral extractions, and asymmetric extractions). In patients with an increase of the irregularity index from T0 to T5, the direction of the displacement of the teeth was assessed. When the displacement was in the direction of the initial situation, it was judged to be relapse. Retainer failures were obtained from the patient files. If the retainer was completely loose, the number of failures was counted as 6.
The dental casts and the intraoral photographs were meticulously inspected for posttreatment changes in the positions of the 6 mandibular teeth (torque difference between 2 adjacent mandibular incisors, or increased buccal inclination and movement of a mandibular canine) as described by Katsaros et al.
One observer (A-M.R.) made all measurements. To determine the measurement error and assess the intraobserver and interobserver agreement of both the intercanine distance and the irregularity index, a random sample of 80 dental casts of 20 patients was, after calibration, evaluated by the main observer (A-M.R.) and a second observer (A.R.). The 2 observers measured the 80 casts twice, with 4 months between the first and second measurements. Angle classification, sagittal contact of the incisors, failures, and relapse were assessed twice by 1 observer (A-M.R.).
Statistical analysis
Descriptive statistics with means and standard deviations were used to report the findings at Ts, T0, T2, and T5. Box plots were made for visual representations of the distributions of intercanine distances. Cross tabs and chi-square tests were used to analyze the relationships between bonding failures and the increments of the irregularity index.
For all nominal variables, the reliability of the measurement was expressed by using the kappa statistic. For the continuous variables (intercanine distances at all time points and irregularity index at Ts), the reliability coefficient (calculated by the Pearson correlation coefficient) and the duplicate measurement error were determined. For these variables, the mean differences between the measured and remeasured variables were analyzed with the paired t test.
At time T0 and later, nearly all subjects had an irregularity index of 0. Therefore, for those time points, the measurement error was expressed by using the kappa statistic, for a dichotomized (0 or >0) irregularity index.
Results
The analysis of intraobserver and interobserver performance for the continuous variables showed high reliability coefficients (0.977 or higher). The duplicate measurement errors for the intercanine distances ranged between 0.15 and 0.25 mm. For the irregularity index, the duplicate measurement errors were 0.34 mm (intraobserver) and 0.47 mm (interobserver). In 2 cases for interobserver performance, a significant difference between observers was found: 0.18 mm for intercanine distance at T0 and 0.14 mm for intercanine distance at T5. For all nominal variables, no measurement error was found; ie, all kappa values, for both intraobserver and interobserver, were equal to 1.
In the total sample, 75 patients (33.9%) were boys, and 146 (66.1%) were girls. The distribution of the Angle classifications at Ts was 25 Class I, 191 Class II, and 5 Class III patients. The mean ages were 13.4 years (SD, 4.2) at the beginning of orthodontic treatment and 16.3 years (SD, 4.2) at the end of treatment. The mean treatment duration was 2.9 years (SD, 0.9). The distribution of the extraction categories was 151 nonextraction subjects (68.3%), 35 (15.9%) with extraction of 1 premolar in every quadrant, 21 (9.5%) without extraction in the mandibular arch and extraction of 1 premolar or first molar in both maxillary quadrants, and 14 (6.3%) in the rest group.
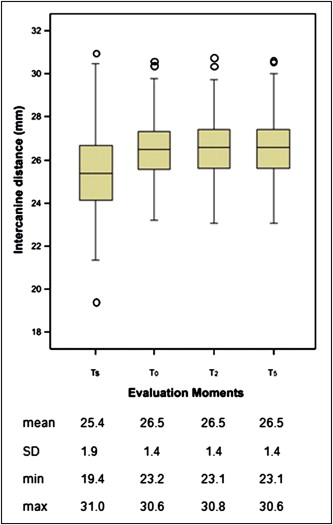
The intercanine distances at Ts, T0, T2, and T5 are shown in Figure 3 . As a result of orthodontic treatment, the mean intercanine distance increased by 1.1 mm: from 25.4 mm at Ts to 26.5 mm at T0. The mean values of the intercanine distance remained stable at 26.5 mm at T2 and T5.
The irregularity index values at all stages are shown in Table I . At the left, the irregularity index values for the whole sample are presented; at the right, the values of subjects with an increase in irregularity from T0 to T5 are presented. The mean irregularity index was 5.35 mm (SD, 3.47) at Ts; it dropped to 0.07 mm (SD, 0.23) at T0 and increased to 0.13 mm (SD, 0.34) at T2. From T2 to T5, the mean irregularity index increased to 0.15 mm (SD, 0.36). Chi-square tests were used to test for differences in the distribution of patients with or without an irregularity index greater than 0 at the 3 time points. This showed that, only for the interval T0 to T5, the increase in the number of patients with an irregularity index greater than 0 was significant ( P = 0.023 for T0-T5, P = 0.162 for T0-T2, and P = 0.452 for T2-T5).
| Time | n | Mean | Minimum | Maximum | SD | n with index >0 |
|---|---|---|---|---|---|---|
| Values for all subjects | ||||||
| Ts | 221 | 5.35 | 0.50 | 16.78 | 3.47 | 221 |
| T0 | 221 | 0.08 | 0.00 | 1.25 | 0.23 | 24 |
| T2 | 221 | 0.13 | 0.00 | 2.50 | 0.34 | 35 |
| T5 | 221 | 0.15 | 0.00 | 2.50 | 0.36 | 42 |
| Values for subjects with increased irregularity from T0 to T5 | ||||||
| Ts | 21 | 5.61 | 1.23 | 11.28 | 2.93 | |
| T0 | 21 | 0.07 | 0.00 | 0.50 | 0.18 | |
| T2 | 21 | 0.61 | 0.00 | 2.50 | 0.68 | |
| T5 | 21 | 0.88 | 0.50 | 2.50 | 0.55 | |
At T0, 197 patients (89.1%) had an irregularity index value of zero, and 24 (10.9%) had values of 0.50 to 1.25 mm. At T2, the alignment of the mandibular front teeth was stable in 207 patients (93.7%); in 14 patients (6.3%) an increase of the irregularity index was measured. At T5, the situation was stable in 200 patients (90.5%) and in 21 patients (9.5%), a mean increase of 0.81 mm (SD, 0.47) was observed. The frequencies of the increments of the irregularity index from T2 to T0, T5 to T2, and T5 to T0 are given in Table II .
| Increment (mm) | Frequency from T2-T0 | Frequency from T5-T2 | Frequency from T5-T0 |
|---|---|---|---|
| 0.00 | 207 | 213 | 200 |
| 0.50 | 9 | 5 | 12 |
| 0.75 | 1 | 0 | 1 |
| 1.00 | 2 | 2 | 5 |
| 1.25 | 0 | 1 | 1 |
| 2.00 | 2 | 0 | 2 |
| Total with increment >0.00 mm | 14 | 8 | 21 |
In the group of patients whose irregularity index increased from T0 to T5 (n = 21), in 5 patients (23.8%), this irregularity was not in the direction of the initial condition, but, in 16 patients (76.2%), the irregularity was in the direction of the initial irregularity.
The numbers and distributions of bonding failures for the time periods are shown in Table III . At T5, 151 patients (68.3%) had never had a bonding failure of their retainer, whereas 70 patients (31.7%) had at least 1 bonding failure of their retainer. In Table IV , the distribution of failures per tooth is shown. The number of bonding failures of the incisors was, compared with the number of bonding failures of the canines, significant lower ( P <0.001). The difference between the number of bonding failures of the central and lateral incisors was not significant ( P = 0.28).


