Introduction
A quantitative assessment of maxillary first molar distalization with and without the maxillary second molar (M2) was carried out.
Methods
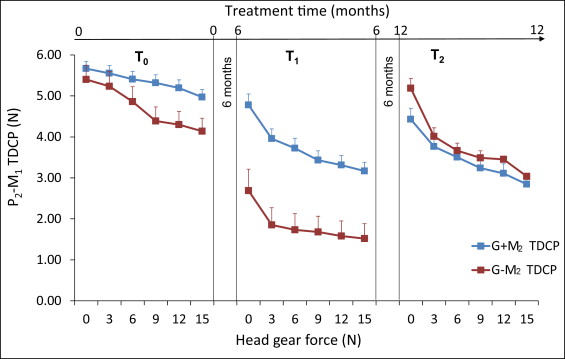
Fifty-six cervical headgear patients undergoing fixed appliance orthodontic treatment were divided into 2 groups: before (G − M2) and after (G + M2) eruption of the maxillary second molars (ages, 11.87 ± 1.20, and 13.05 ± 1.55 years, respectively). The tightness of the dental contact point (TDCP) and the space between the second premolar and the maxillary first molar were measured at 6 levels of headgear force (0-15 N) at 3 intervals 6 months apart (T0, T1, T2).
Results
Relationships were found between space and TDCP, time, and presence or absence of the maxillary second molar at T1 and T2 ( P <0.001). The TDCP decreased and space increased with increase in initial headgear force. An increase in initial force beyond 6 to 9 N did not significantly increase the initial maxillary first molar distalization. The G − M2 TDCP and space measurements were similar to those of G + M2 at T2 with the eruption of the maxillary second molar. From T0 to T1, maxillary first molar distalization was greater in G − M2. In comparison with our previous headgear-alone study, initial distalization with a fully bonded appliance was reduced by 4-fold.
Conclusions
Headgear therapy is more effective before the eruption of the maxillary second molar. Once it erupts, the distalization pace of the maxillary first molar is reduced, but it can nevertheless be pursued at a slower pace when the maxillary second molar is present.
Highlights
- •
Headgear treatment was evaluated at different force levels.
- •
Distalization in the absence or presence of the maxillary second molars was assessed.
- •
Distalization was measured with tightness of dental contact point and space gauges at 3 time points.
- •
Headgear therapy is more effective before the eruption of the second molars.
- •
The initial effective headgear force level is 3 to 6 N and should not exceed 9 N.
It is an accepted treatment modality to direct extraoral forces through the maxillary permanent first molar to cause its distalization via headgear (HG). However, this effect can vary considerably under different HG loading conditions as well as in the presence or absence of teeth distal to the maxillary permanent first molar. The presence of the second molar (M2) and third molar in different developmental and eruptive stages can also act as a physical impediment to the extent and direction of maxillary permanent first molar distalization.
Kloehn advocated early HG treatment to distalize the maxillary teeth into correct occlusion with the mandibular dentition. It has also been proposed that treatment of Class II malocclusions should be performed before the eruption of the maxillary permanent second molars and canines, since the latter might affect treatment efficiency. Previous studies with noncompliance appliances have reported that before maxillary second molar eruption, the maxillary first molar can be distalized by 1 to 2 mm per month with little anchorage loss—ie, forward displacement of the anterior segment. It has been shown when using the pendulum appliance that once the maxillary second molars have erupted, distal movement of the maxillary first molar is slowed, and anchorage loss is more common, producing mesial movement of the anterior teeth. Ten Hoeve and Jeckel and Rakosi concluded that distalization of the maxillary permanent first molar is restrained by the maxillary second molar; consequently, they recommended distalization before second molar eruption. Similar findings have been reported for several intraoral molar distalization appliances.
On the other hand, Muse et al, using a Wilson rapid molar distalization appliance, and Ghosh and Nanda, using the pendulum appliance, found that the presence of the maxillary second molar did not significantly affect the rate of first molar movement. Additional studies with repelling magnets and the pendulum appliance support the latter claims of the minor effect of the maxillary second molar on first molar distalization. This diversity could be related to the interrupted force regimen produced by HG compared with the continuous force of noncompliance appliances.
In a previous study, we demonstrated that an incremental increase in cervical HG force, applied per se, caused differences in the gap created between the maxillary first molar and the second premolar, and that first molar distalization was influenced by the absence or presence of the maxillary second molar. In this study, we investigated whether similar effects on molar distalization can be expected when HG traction is applied during full-arch fixed appliance therapy and over a longer period of time. Furthermore, we investigated whether HG therapy is affected by short-term (initial periodontal ligament [PDL] reaction to HG placement) and long-term (bone remodeling) changes, and we determined the range for the initial HG force.
With respect to the latter, few previous studies have examined this issue, mostly describing the orthopedic effects of diverse HG forces. For example, Zentner et al studied orthopedic forces of 5.6 N (Newton = 101.97 gram-force = 3.597 oz) vs orthodontic forces of 3.5 N on a macerated human skull using holographic interferometry. They reported that lower HG forces produced significantly greater deformations than did higher forces; this indicates that there might be an upper limit to the optimal force level.
Dental changes caused by HG therapy have been reported in the literature. Andreasen and Johnson applied diverse forces in each side and found that over a 12-week period the molar receiving 4 N of HG force distalized 2.5 times more than did the other molar, which received 2 N of force. After 8 weeks in the 2-N side, no further increase in molar distalization was found, whereas the 4-N side demonstrated continuation of molar distalization at the same pace to end of the study (12 weeks). This suggests that there might be a lower limit to the optimal force level.
The objectives of this study were to evaluate HG distalization efficacy concomitant with edgewise fixed appliance treatment in relation to 4 variables: the absence or presence of the maxillary second molar, the amount of distal movement of the maxillary first molar, the magnitude of the HG force, and maxillary second molar eruption.
The null hypotheses were that at all stages of treatment, the amount of distalization of the maxillary first molar is not affected by the presence or absence of the maxillary second molar, and the initial force magnitude has no effect on initial maxillary first molar distal displacement.
Material and methods
The study sample comprised 56 patients presenting for treatment at the Department of Orthodontics, University of Tel Aviv in Israel, diagnosed as having an Angle Class II malocclusion and treated without extractions with cervical HG for at least 1 year for a minimum of 12 hours per day. Subjects were included in the study when part of their malocclusion was related to maxillary dentoskeletal protrusion (SNA, >83°; mean, 85.9° ± 2.03°). Syndromic patients (eg, cleft lip) were excluded, as were those with early mesial drift of the maxillary first molar (eg, congenitally missing second premolar) and adults (age, >16.5 year). The Class II severity ranged from a half-step to a full-step molar relationship. All treatments included the use of fully bonded edgewise appliances without intermaxillary or intramaxillary elastics. Data were gathered at 3 time points: T0, start of HG therapy; T1, 6 months after T0; and T2, 12 months after T0.
The sample was divided into 2 groups: (1) G − M2: both maxillary second molars were unerupted at T0 or showed both clinically and radiographically no contact point between the first and second molars (21 subjects: 9 boys, 12 girls; mean age, 11.87 ± 1.20 years), and (2) G + M2: at T0, both maxillary second molars were present in the oral cavity, with both clinically and radiographically an interproximal contact point between the first and second molars (35 subjects: 18 boys, 17 girls; mean age, 13.05 ± 1.55 years).
In addition to determining the presence or absence of the second molars, we examined the Nolla stage of maxillary second molar development radiographically.
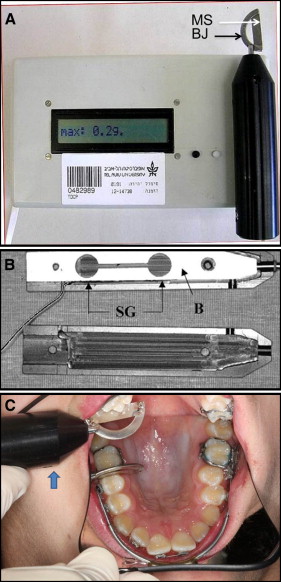
A 0.022 × 0.028-in preadjusted appliance was bonded to the maxillary dentition, into which was inserted an uncinched nickel-titanium archwire. The archwires were changed according to the progress in leveling, from 0.014 to 0.018 in. A Kloehn type of cervical HG was delivered to the bands on the permanent first molars. The HG consisted of a medium outer bow, with “U” loops (3M Unitek, Monrovia, Calif); the outer arm was positioned horizontally (with no adjusted upward tilt). The HG force was increased gradually from 0 to 15 N in 3-N increments (0, 3, 6, 9, 12, and 15 N). Zero reflected the measurement when the facebow was inserted in the mouth without attaching the (activation) neck strap. Upon activation, the force created by the neck strap was measured by a force gauge (weighing scale, spring type WS072; Narang Medical, New Delhi, India) ( Fig 1 ). Displacement of the maxillary right first molar was measured by 2 direct methods at T0, T1, and T2. The first method was as a function of the change in tightness of the contact point between the second premolar and the first molar using the tightness of dental contact point (TDCP) device, according to the method of Vardimon et al ( Fig 2 , A ). Briefly, the device measures the amount of force required to insert a metal strip (0.15 mm) between 2 adjacent dental contact points in TDCP units ( Fig 2 , B ). The TDCP was measured on the right side and could be measured as long as the maxillary first molar displacement was smaller than 0.15 mm.

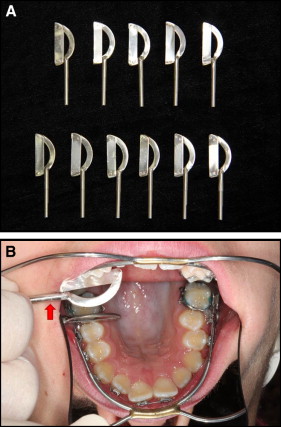
In the second method, custom-made metal gauges (leaves) were inserted at the contact point of the second premolar and the first molar in serial fashion. The gauges (made at workshop of the Faculty of Physics, Tel Aviv University) differed in thickness from 0.1 to 0.6 mm, in 0.05-mm increments (totaling 11 gauges) ( Fig 3 ). Displacements less than 0.1 mm were considered to be no displacement. Each of the 2 methods was measured while the subject was seated in a dental chair reclined to 135°, and the HG force was increased gradually. The total time for TDCP and space measurements for the 6 force magnitudes was about 12 minutes. The measurements were taken continuously. All measurements were taken by the same investigator (Y.M.). The average HG force worn by the patient during the 12 hours of wear was 4 N.
Statistical analysis
The random errors (calculated using the Dahlberg formula ) and the systematic error (calculated using a paired t test) of the 2 instruments were examined on 5 subjects from each group; the 2 sets of measurements were taken at 1-week intervals.
The Dahlberg formula is the following. D=√∑Ni=Id2i2N
D = ∑ i = I N d i 2 2 N
D is the random error, d i is the difference between the first and the second measurements, and N is the sample size that was remeasured.
For repeated measures of the TDCP, the random error was 0.209 N (13%); for the space measurements, it was 0.012 mm (8.6%). The larger error calculated in the former was caused by stretching of the PDL during the initial TDCP measurements; this affected subsequent measurements. Therefore, only the first TDCP measurements were considered. No significant differences were found in the paired t tests between the first and second measurements, confirming the absence of systematic error.
Analysis of variance (ANOVA) with repeated measures with the post hoc Tukey test was used to analyze each parameter (TDCP and space), where the HG force (0-15 N) and time (T0, T1, T2) were within factors, and maxillary second molar presence or absence (G + M2, G − M2) was the between factor. Since the TDCP values did not show a normal distribution, the formula 1/(7 − TDCP) was used to normalize the results: 7 reflects the maximum TDCP value (in Newtons) that can be registered by the TDCP device.
Pearson correlation analysis was used to analyze the correlations between TDCP and space for each time point at all HG forces.
Results
Nolla stages of maxillary second molar development were 7.6 ± 0.5 (1/3 to 2/3 of the root was completed) for G − M2 and 9.5 ± 0.5 (root completed with open or closed apex) for G + M2. These values correspond to previous studies.
At T0, there was no significant difference in TDCP between G + M2 and G − M2. At no HG load force (0 N), the 2 groups had similar contact point tightness. In both groups, a nonsignificant decrease in contact point tightness was found as the HG force was increased; however, the decrease was greater in subjects without the second molar (G − M2) ( Fig 4 ).