Introduction
Orthodontists have used various compliance-dependent physical means such as headgears and intraoral appliances to prevent anchorage loss. The aim of this study was to determine whether 1 local application of the bisphosphonate zoledronate could be used to prevent anchorage loss during extraction space closure in rats.
Methods
Thirty rats had their maxillary left first molars extracted and their maxillary left second molars protracted into the extraction space with a 10-g nickel-titanium closing coil for 21 days. Fifteen control rats received a local injection of phosphate-buffered saline solution, and 15 experimental rats received 16 μg of the bisphosphonate zoledronate. Bisphosphonate was also delivered directly into the extraction site and left undisturbed for 5 minutes. Cephalograms and incremental thickness gauges were used to measure tooth movements. Tissues were analyzed by microcomputed tomography and histology.
Results
The control group demonstrated significant ( P <0.05) tooth movements throughout the 21-day period. They showed significantly greater tooth movements than the experimental group beginning in the second week. The experimental group showed no significant tooth movement after the first week. The microcomputed tomography and histologic observations showed significant bone loss in the extraction sites and around the second molars of the controls. In contrast, the experimental group had bone preservation and bone fill. There was no evidence of bisphosphonate-associated osteonecrosis in any sample.
Conclusions
A single small, locally applied dose of zoledronate provided maximum anchorage and prevented significant bone loss.
Orthodontic tooth movements can have undesirable effects on the surrounding teeth. The challenge is to design a force system that maximizes desirable tooth movements and simultaneously minimizes anchorage loss. Traditional methods to mitigate anchorage loss include headgears, various intraoral appliances, and elastics, all of which depend on patient compliance. Without compliance, anchorage is often lost, causing an increase in treatment time and a risk of adverse effects, such as root resorption, white spot lesions, caries, gingivitis, and compromised treatment results.
Currently, miniscrew implants are the preferred method of providing maximum anchorage because they are small, are relatively uncomplicated to place, and provide an effective mechanical means of preserving anchorage. Although miniscrew implants provide excellent skeletal anchorage, they have highly variable success rates and do not always remain stable throughout treatment.
In lieu of mechanical means, pharmacologic methods hold great potential for providing anchorage. A recent pharmacologic method to reduce anchorage loss has targeted the receptor activator of nuclear factor kappa B ligand (RANKL), a key pathway in bone metabolism. Common medications such as nonsteroidal anti-inflammatory drugs have been shown to inhibit orthodontic tooth movement by interrupting the cell signals between the periodontal ligament, tooth, and bone that are responsible for regulating bone resorption. The nonsteroidal anti-inflammatory drugs’ effects on orthodontic tooth movement primarily are considered side effects; they have not been used clinically to inhibit orthodontic tooth movement.
The newest pharmacologic agents available for decreasing orthodontic tooth movement are the bisphosphonates, a class of synthetic drugs that limits bone resorption by inhibiting osteoclastic activity. Bisphosphonates are typically used to treat diseases of the bone such as osteoporosis, Paget’s disease, multiple myeloma, and metastatic bone cancer. Bisphosphonates are divided into 2 families: simple (nonnitrogen-containing) bisphosphonates and nitrogen-containing bisphosphonates. Various configurations of nitrogen-containing bisphosphonates create substantial increases in potency. The nitrogen-containing bisphosphonates first introduced (eg, pamidronate [Aredia] and aledronate [Fosamax]) were 10 to 100 times more potent than the simple nonnitrogen-containing bisphosphonates (eg, etidronate [Didronel]). The newest class of nitrogen-containing bisphosphonates has a heterocyclic ring (eg, zoledronate [Zometa]) and is up to 10,000 times more potent than etidronate.
Because of their effects on bone resorption, the clinical applications of bisphosphonates have been investigated in orthopedic surgery and dentistry. Bisphosphonate-coated orthopedic implants have significantly increased the mechanical fixation of orthopedic implants, accelerated the healing of fractures, improved fixation and bone volume surrounding orthopedic screws, and improved the stability of joint replacements. Bisphosphonates also have been used to treat periodontitis in rats and to prevent bone loss after mucoperiosteal flap surgery in rats. Bisphosphonates have been shown to reduce bone resorption, root resorption, ankylosis, and pulpal mineralization of reimplanted rat teeth after avulsion. They have recently been used to decrease skeletal relapse after maxillary expansion and mandibular distraction.
In orthodontics, bisphosphonates have been shown to reduce root resorption during tooth movements in rats. Bisphosphonates have also been used to decrease anchorage loss and postorthodontic relapse in rats. Two studies reported cessation of tooth movement in the experimental groups after the first week, and 3 others reported continued movement throughout the experiments. No previous study has demonstrated cessation of tooth movement with zoledronate. More importantly, the effects of bisphosphonates with the added strain on anchorage caused by tooth extraction has not been investigated.
The purpose of this study was to determine whether local application of the bisphosphonate zoledronate can provide maximum anchorage for extraction space closure in rats. Zoledronate was used because it is the most potent bisphosphonate available and has one of the highest bone affinities of all the bisphosphonates. These favorable pharmacokinetic characteristics should enable small doses of zoledronate to be used locally to minimize anchorage loss and unwanted side effects.
Material and methods
A power analysis based on a conservative estimate of the standard deviations (0.6 mm) and effect sizes (0.7 mm) of orthodontic tooth movement previously reported in studies evaluating bisphosphonates showed that 15 rats per group were needed to obtain a power of 87% with an alpha at 5%. On that basis, 15 rats were randomly allocated to the experimental group, and 15 were allocated to the control group. Retired breeder adult male Sprague-Dawley rats (Harlan Laboratories, Indianapolis, Ind) were used and treated ethically in compliance with the regulations at Baylor College of Dentistry at Texas A&M Health Science Center in Dallas. The animals were acclimatized for at least 3 days before the experiment. They were fed a soft diet consisting of powdered rat chow (Harlan Laboratories), DietGel Recovery (ClearH 2 0, Portland, Me), HyrdoGel (ClearH 2 0), and water ad libitum, and were maintained in a room at 25°C with a 12-hour light and dark cycle. The animals were weighed at baseline (day 0) and every 7 days (days 7 and 14) until they were killed on day 21. A 21-day experimental period was chosen based on previous studies of tooth movements in rats.
After they were weighed, the rats were anesthetized with an intraperitoneal injection of xylazine (10 mg/mL), ketamine (100 mg/mL), and acepromazine (1 mg/mL). A 50-μL solution of phosphate-buffered saline, containing 16 μg of zoledronate (pH 7.0) or an equal volume of phosphate-buffered saline solution (pH 7.1) containing no zoledronate was injected into the experimental and control rats, respectively, by using a 3/10-mL syringe. The drug was injected by an operator (A.J.O.) who was blinded as to the contents of the syringes at 2 separate times to ensure that the bone adjacent to the tooth was adequately covered. Approximately one third of the solution was injected into the mesiopalatal and distopalatal aspects of the maxillary left second molar and the vestibule above the first molar. The maxillary left first molars of both the control and the experimental groups were then extracted by luxating the tooth with a 20.5-gauge needle. Accessible residual tooth roots were removed with a dental explorer. Great care was taken in removing the root tips; the root tips were left in place if it appeared that there was risk of damaging the bone in the extraction site. After extraction, another one third of the solution was injected into the same sites. The last one third of the solution was injected into the extraction site and left undisturbed for 5 minutes before appliance placement. A 1-minute lavage of zoledronate has been previously shown to be adequate ; 5 minutes was chosen as the time to ensure adequate coverage and absorption into bone. Because of possible systemic effects of the zoledronate, no treatment was performed on the contralateral side.
An 0.008-in-diameter steel ligature was passed between the contact of the maxillary left second and third molars and twisted approximately 3 times to ensure that it was secure, but not tight, against the mesial aspect of the second molar. A 10-g closed-coil nickel-titanium spring (G&H Wire, Franklin, Ind; 0.006-in wire, 0.025-in lumen, 7 mm) was then attached to a free end of the steel ligature. The steel ligature was passed through the lumen of the spring at approximately the third coil to ensure adequate strength. Small retention grooves were cut into both maxillary central incisors (distofacially and distolingually) with a high-speed hand piece and a carbide bur. The mandibular incisors were trimmed weekly with a coarse diamond bur to ensure that they were out of occlusion and not at risk of breaking the appliance.
Another 0.008-in-diameter steel ligature was inserted into the free end of the spring at approximately the third coil, wrapped around the retention grooves on the maxillary central incisors, twisted, and cut to lie flat in the facial embrasure between the central incisors. Transbond (3M Unitek, Monrovia, Calif) self-etching primer was applied to the mesial and lingual surfaces of the second molar. Just enough Transbond XT (3M Unitek) was applied to the mesial and lingual surfaces to cover the wire and prevent it from slipping off the tooth. The cut end of the steel ligature was covered with a small amount of Transbond XT to prevent ulceration of the soft tissues. To ensure that the second and third molars were not inadvertently bonded together, free movement of the molars was confirmed with an explorer. One pediatric mandibular incisor stainless steel crown (3M Unitek) was cemented over the maxillary incisors with band cement (3M Unitek). Extra cement was added to the lingual surfaces to protect the spring from the mandibular incisors during mastication. All cements were cured according to manufacturer’s instructions by using a curing light. The same operator (A.J.O.) placed all appliances.
This appliance design provided 21 days of constant protraction of the maxillary left second molar into the extraction site of the first molar. One control appliance failed within the first week of placement and was immediately replaced.
Follow-up measurements were made every 7 days after appliance placement. The rats were anesthetized in a chamber with 3% isofluorane at a flow rate of 2 L/min of oxygen. Then the mandibular incisors were retrimmed with the diamond bur, and the appliances and soft tissues were checked. The rats always recovered from the anesthesia under an infrared thermal heater.
A cephalostat was used to ensure a constant distance of 6 in from source to sensor. Digital lateral cephalograms were taken with an x-ray unit (Intra; Planmeca U.S.A., Roselle, Ill) set at 60 kV and 6 mA for 0.080 seconds. A 10-mm metal bar was secured to the sensor to calibrate the images. Lateral radiographs were taken immediately after appliance placement and at 7, 14, and 21 days after appliance placement.
The animals were killed on day 21. They were anesthetized as on the day of appliance placement and killed by exsanguination. The tissues were fixed with 10% formalin. The mandibles were carefully dissected from the maxillae after decapitation. Photographs were taken, and the maxillae were stored in 10% formalin for the analyses.
The radiographs were randomized, and 1 operator (A.J.O.), blinded to group affiliations, made all measurements with imaging software (ImageJ, National Institutes of Health, Bethesda, Md) after calibrating each image with the 10-mm radiopaque bar.
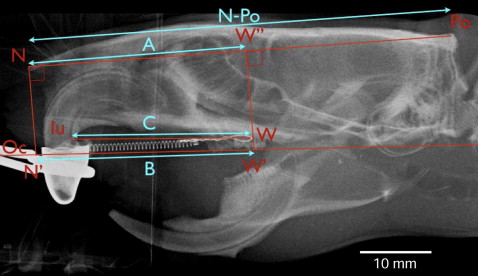
Nasion (N, most anterior point on the nasal bone) and porion (Po, most posterior and superior point on the skull) were identified on each radiograph ( Fig 1 ) by using landmark definitions previously described. The lines N-Po and occlusal plane were drawn, and a perpendicular line was constructed from N to intersect the occlusal plane (N′). A line perpendicular to N-Po was constructed through the most distal point of the wire (W) until it intersected the occlusal plane (W′). Measurement A was the distance N to a perpendicular from N-Po through W, measurement B was the distance N′-W′, and measurement C was the distance from the most anterior-inferior point on the maxilla posterior to the incisors to W. Duplicate measurements were made by a blinded operator (A.J.O.), and the averages of the 2 measurements were used for the statistical analyses.
After the rats were killed, gross interdental tooth movements were measured by a blinded operator (A.J.O.) with incremental thickness gauges (Align Technologies, Santa Clara, Calif). The gauges were 0.10, 0.20, 0.25, 0.30, 0.40, or 0.50 mm thick. To measure total tooth movement from baseline to day 21, the gauges were placed between the contact points of the maxillary left second and third molars. The thickest gauge or combination of gauges that could be inserted without moving the teeth was used and recorded. If the 0.10-mm gauge did not fit between the teeth, 0.0 mm of movement was recorded. Two measurements were taken for each animal and averaged.
Three animals from both the control and experimental groups were randomly chosen for microcomputed tomography and histologic analyses. The steel ligature was removed from the second molar, and the section of the alveolus from the distal aspect of the third molar to the mesial aspect of the extraction site was excised with a thin diamond table saw. The samples measured approximately 15 × 5 × 5 mm. The samples were scanned with microcomputed tomography (model 35; Scanco Medical, Basserdorf, Switzerland) with an isotropic resolution of 12 μm. X-ray energy levels were set to 55 kVp, the current was set to 145 μA, and the integration time was 400 ms.
The same 6 samples were then decalcified in 0.5 mol/L of EDTA in a microwave (24°-27°C) for 3 weeks. After decalcification, the samples were dehydrated, embedded in paraffin, and sectioned by using conventional methods at a thickness of 6 μm. The samples were stained with Harris hematoxylin and eosin Y alcohol (H&E stain) and mounted on glass slides for evaluation.
Statistical analysis
By using statistical software (SPSS, Chicago, Ill), intraexaminer reliability was evaluated based on comparisons of 120 replicate measurements. Systematic errors, evaluated by using Wilcoxon tests, ranged from –0.0033 to –0.0298 mm and were not statistically significant. Method error, quantified with the method error statistic (√Σd2/2n), ranged from 0.0295 to 0.0316 mm. Single measures intraclass correlations ranged from 0.997 to 0.999. Intergroup comparisons were analyzed with the Mann-Whitney test, and changes over time were evaluated with Wilcoxon tests.
Results
There was no statistically significant difference in weights between the groups at baseline. The experimental group did show significantly greater weight gains during the second week (days 7-14) than did the control group ( Table I ). There were no other statistically significant group differences in weight over time. At day 21, the controls returned to their initial weights; the experimental animals finished 21 g heavier than their initial weights, but the group differences at day 21 were not statistically significant ( P = 0.098).
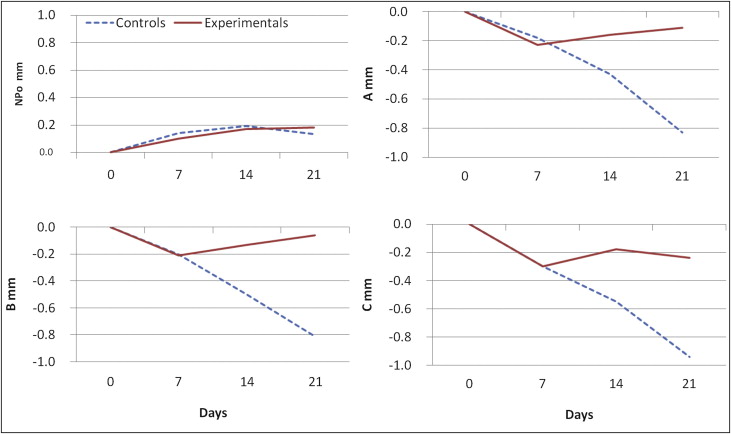
Line N-Po showed slight increases (<0.2 mm) over the experimental period, but no changes that occurred over time were statistically significant for either the control or the experimental group ( Table II ; Fig 2 ). Both group exhibited statistically significant initial (baseline-day 7) tooth movements, with no significant group differences. The controls had statistically significant decreases in space for all 3 measurements (A, B, and C) over every time interval. For the experimental animals, measurement A demonstrated significant movements from baseline to day 14 and from baseline to day 21; these were due to the initial changes (baseline-day 7); the changes from days 7 to 14 and 14 to 21 were small and not statistically significant. With the exception of the initial change (baseline-day 7), no other changes of measurement B were statistically significant. The experimental animals had an initial decrease in measurement C, followed by a statistically significant increase in space between days 7 and 14. The significant decreases in space that occurred in measurement C from baseline to day 14 and from baseline to day 21 were again due to the initial (baseline-day 7) changes. There were consistent and statistically significant group differences in tooth movements for measurements A, B, and C over days 7 to 14, days 14 to 21, baseline to day 14, and baseline to day 21. There was also a statistically significant difference between the groups for the gross interdental tooth measurements, with the control and experimental animals averaging 0.62 and 0.07 mm of separation, respectively.
| Days | Control animals | Experimental animals | Group differences | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | P | |
| Measurement N-Po | |||||
| 0-7 | 0.14 | 0.43 | 0.10 | 0.45 | 0.870 |
| 7-14 | 0.05 | 0.34 | 0.07 | 0.32 | 0.895 |
| 14-21 | −0.06 | 0.32 | 0.01 | 0.42 | 0.575 |
| 0-14 | 0.19 | 0.40 | 0.17 | 0.31 | 0.870 |
| 0-21 | 0.13 | 0.39 | 0.18 | 0.46 | 0.838 |
| Measurement A | |||||
| 0-7 | −0.18 ∗ | 0.24 | −0.23 ∗ | 0.36 | 0.780 |
| 7-14 | −0.21 ∗ | 0.17 | 0.07 | 0.27 | 0.002 |
| 14-21 | −0.40 ∗ | 0.30 | 0.05 | 0.28 | <0.001 |
| 0-14 | −0.43 ∗ | 0.29 | −0.168 ∗ | 0.31 | 0.021 |
| 0-21 | −0.83 ∗ | 0.45 | −0.118 ∗ | 0.23 | <0.001 |
| Measurement B | |||||
| 0-7 | −0.20 ∗ | 0.28 | −0.21 ∗ | 0.39 | 0.847 |
| 7-14 | −0.25 ∗ | 0.17 | 0.08 | 0.25 | <0.001 |
| 14-21 | −0.31 ∗ | 0.25 | 0.07 | 0.28 | 0.001 |
| 0-14 | −0.50 ∗ | 0.29 | −0.13 | 0.28 | 0.002 |
| 0-21 | −0.81 ∗ | 0.45 | −0.06 | 0.28 | <0.001 |
| Measurement C | |||||
| 0-7 | −0.30 ∗ | 0.21 | −0.30 ∗ | 0.25 | 0.561 |
| 7-14 | −0.22 ∗ | 0.17 | 0.13 ∗ | 0.17 | <0.001 |
| 14-21 | −0.38 ∗ | 0.31 | −0.06 | 0.18 | 0.002 |
| 0-14 | −0.55 ∗ | 0.27 | −0.18 ∗ | 0.18 | <0.001 |
| 0-21 | −0.94 ∗ | 0.45 | −0.24 ∗ | 0.21 | <0.001 |
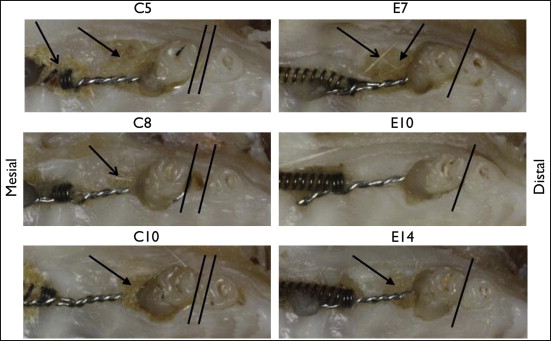
Both groups showed signs of delayed healing or ulcers at the extraction sites, but there were no clinical signs of osteonecrosis ( Fig 3 ). There were no signs of infection or exposed necrotic bone in any of the 30 animals. In the control animals, a diastema developed between the mesial aspect of the third molar and the distal aspect of the second molar. Diastemas did not develop in the experimental animals. Retained food debris and hair were found around the appliances and in the extraction sites in some control and experimental animals. Compared with the untreated side, there appeared to be some mesial movement of the third molar on the treated side of the control group, and the alveolar bone on the experimental side at the extraction site of the controls appeared to be wider and higher than the bone on the untreated side.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


