Lipids
The Condensed Energy
• Describe how fatty acids affect the properties of fat.
• Explain the functions of fats in the body and how these affect oral health.
• Identify dietary sources for saturated, monounsaturated, polyunsaturated, omega-3 and trans fatty acids, and cholesterol.
• Calculate the recommended amount of dietary fat.
• Plan appropriate interventions when dietary modification of fat intake has been recommended to a patient.
 Test Your NQ
Test Your NQ
1. T/F No food containing more than 35% of its kilocalories from fat can be considered healthy.
2. T/F Fats containing vitamin E deteriorate and become rancid rapidly.
3. T/F A product containing more unsaturated fatty acids than saturated fatty acids is a healthier food choice than one containing a higher proportion of saturated fatty acids.
4. T/F Dietary fat intake should be less than 20% of total kilocalories.
5. T/F Bananas and avocados contain cholesterol.
6. T/F Oils are less fattening than solid fats.
7. T/F Fat intake has been linked more frequently to cancer than any other dietary factor.
8. T/F Nuts and cheeses are nutritious foods that should be recommended to all patients for snacks because they reduce the rate of caries.
10. T/F Omega-3 fatty acids are polyunsaturated fatty acids.
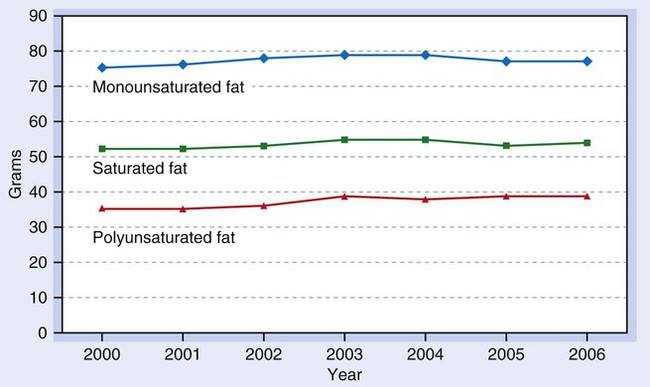
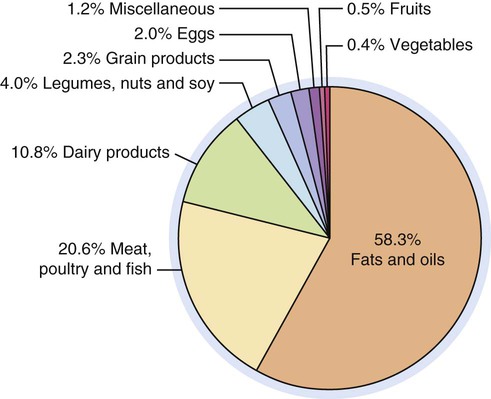
Added fats and oils provide more kilocalories in the average American diet than any other food group. Examination of U.S. food supply trends indicates total fat intake, which remains at a high level, increased slightly since 2000. The trend reflects a very slight increase in fats provided by vegetable oils (Fig. 6-1).1 Between 1977 and 2008, daily consumption of total fat declined from 39.7% to 33.4% of total caloric intake.2 Consumers have become more aware of healthy food choices, but changes in eating patterns are difficult. Food manufacturers, producers, and grocers have responded to concerns by (a) trimming fat from meats, (b) providing leaner cuts of beef and pork, (c) replacing tropical oils and trans fats in processed foods, and (d) manufacturing foods containing less fat. In addition, some consumers have increased their consumption of fish and poultry and substituted lower fat milk for whole milk. The fat content of very lean beef and pork cuts currently compares favorably with a skinless chicken breast. Added fats and oils provide most of the kilocalories Americans consume (Fig. 6-2).
Classification
Fats in the diet should actually be called lipids. Lipids contain the same three elements as carbohydrates: carbon, hydrogen, and oxygen. Lipids contain less oxygen in proportion to hydrogen and carbon than carbohydrates. The structure and function of lipids are covered in detail in Chapter 2 and on the Evolve website. Because of their structure, they provide more energy per gram than either carbohydrates or proteins.
Chemical Structure
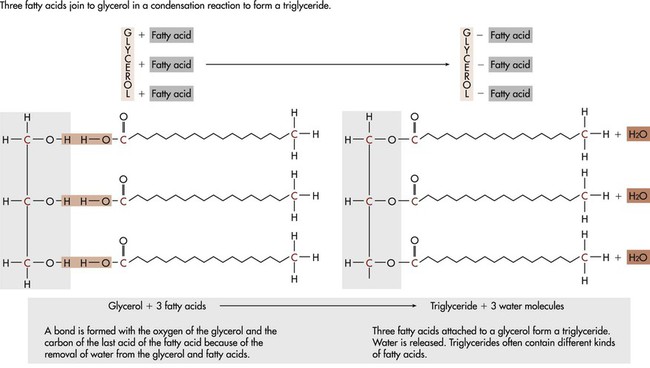
Triglycerides are composed of fatty acids and glycerol, as shown:
< ?xml:namespace prefix = "mml" />



A fatty acid is a chain of carbon atoms attached to hydrogen atoms with an acid grouping on one end. Glycerol is the alcohol portion of a triglyceride to which the fatty acids attach. Triglycerides are the most common fat present in animal or protein foods (Fig. 6-3). Monoglycerides and diglycerides are found in the small intestine and result from the breakdown of triglycerides during digestion. Free fatty acids, monoglycerides, and glycerol can cross cell membranes.
Saturated Fatty Acids
As discussed in Chapter 2, fatty acids are classified according to their degree of saturation. Saturation of a fatty acid depends on the number of hydrogen atoms attached to the carbon chain. Saturated fatty acids (SFAs) contain only single bonds, with each carbon atom having two hydrogen atoms attached to it (see Chapter 2, Fig. 2-15). Palmitic and stearic acids (see Chapter 2, Table 2-4), the two most prevalent SFAs, are structural components of tooth enamel and dentin.
Monounsaturated Fatty Acids
When adjacent carbon atoms are joined by a double bond because two hydrogen atoms are lacking, there is a gap between the hydrogen atoms in the chain; it is called an unsaturated fatty acid. Monounsaturated fatty acids (MUFAs) contain only one double bond (see Chapter 2, Fig. 2-12). The most abundant MUFA is oleic acid. Oleic acid is also a structural component of the tooth.
Trans Fatty Acids
Hydrogenation is a commercial process in which vegetable oil is converted to a solid margarine or shortening by adding hydrogen to the oil. This process results in naturally unsaturated vegetable oils being changed to a SFA by changing unsaturated bonds to saturated bonds. Hydrogenation can be controlled, so “tub” or “soft” margarine is “partially hydrogenated,” or not completely saturated. The hydrogenation process not only increases the proportion of SFAs, but also changes the shape of the fatty acid. When the hydrogen atoms are rotated so that they are on opposite sides of the bond, in the “trans” position (see Chapter 2, Fig. 2-16), the fatty acid is called a trans fatty acid. Partial hydrogenation results in large numbers of fatty acids having this altered shape. Foods with trans fatty acids have a longer shelf life, and flavors are stable. The most common trans fatty acid is elaidic acid, found in partially hydrogenated vegetable oils, such as tub margarines and cooking oils. A naturally-occurring trans fatty acid, vaccenic acid, with double bonds on adjacent carbons, is present in small amounts in milk and meat of ruminants (cows, sheep, and deer). Limited research suggests that these trans fats may possibly have health-enhancing potential.
Polyunsaturated Fatty Acids
When carbons in a fatty acid are connected by two or more double bonds, the fatty acid is polyunsaturated (see Chapter 2, Fig. 2-13). Linoleic acid and arachidonic acid are polyunsaturated fatty acids (PUFAs). These PUFAs are omega-6 fatty acids. Their first double bond is on the sixth carbon from the omega (terminal) end; they are also referred to as n-6 PUFAs.
Omega-3 fatty acids, or α-linolenic acids, make up another class of PUFAs. As shown in Chapter 2, Figure 2-13A, these fatty acids are unique in that the first double bond is located three carbon atoms from the omega end of the molecule; hence they are called omega-3s or n-3s. Omega-3 fatty acids include α-linolenic acid, which has 18 carbon atoms and two double bonds, and eicosapentaenoic acid (EPA), which has 20 carbon atoms and five double bonds.
Characteristics of Fatty Acids
 Dental Considerations
Dental Considerations Nutritional Directions
Nutritional Directions
• Frying foods at low temperatures causes the food to absorb excessive amounts of fats, whereas frying at very high temperatures results in decomposition of some fats, which can be irritating to the intestine, causing gastrointestinal discomfort after meals containing fried foods.
• The relatively small amounts of trans fatty acids that occur naturally in meat and dairy products do not appear to be harmful.
• Butylated hydroxyanisole and butylated hydroxytoluene are antioxidants added to processed foods to retard or prevent spoilage.
Compound Lipids
Phospholipids
Lipoproteins
Lipoproteins are produced by the body to transport insoluble fats in the blood. Lipoproteins are compound lipids composed of triglycerides, phospholipids, and cholesterol combined with protein (see Chapter 2, Fig. 2-18). The liver and intestinal mucosa produce lipoproteins. Four different types of lipoproteins are present in the blood: high-density lipoproteins (HDLs), low-density lipoproteins (LDLs), very-low-density lipoproteins (VLDLs), and chylomicrons.
The ratio of lipid to protein in lipoproteins varies widely; these variations affect their density. Density increases as lipids decrease and protein increases. Lipoproteins can be classified according to their density and composition, as shown in Figure 6-4. Phospholipids in lipoproteins are present in approximately the same proportions in all individuals.
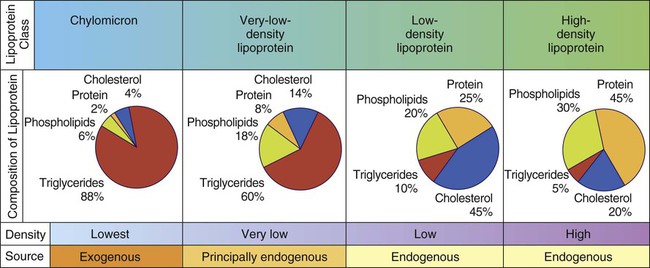
HDLs, which have been thought to protect against development of CHD, contain greater amounts of protein and less lipid. LDL cholesterol typically constitutes 60% to 70% of the total blood cholesterol. It is considered the main agent in elevated serum cholesterol levels, or the “bad” cholesterol. Serum HDL, LDL, and VLDL are important predictors of heart disease, as discussed in Health Application 6.
Cholesterol
Cholesterol is a fatlike, waxy substance classified as a sterol derivative with a complex ring structure (see Chapter 2, Fig. 2-17). More details on the structure and function of cholesterol are available online in the Evolve website. Because the body frequently produces more cholesterol than it absorbs, cholesterol intake is not essential. Cholesterol has important functions as a constituent of the brain, nervous tissue, and bile salts; a precursor of vitamin D and steroid hormones; and a structural component of cell membranes and teeth. Lipoproteins transport cholesterol in the blood.
Physiological Roles
Energy
Palatability
Fats contribute to the palatability and flavor of foods. In cooking, they improve texture. A receptor on the tongue and a potential pathway for detection of a “fatty taste” has been identified, which may affect food preferences.3,4 Preference for high-fat foods develops at an early age and persists through adulthood.
Complementary Relationships
Linoleic acid, an omega-6 fatty acid with 18 carbon atoms and two double bonds (see Chapter 2, Fig. 2-12), cannot be synthesized by the body and must be supplied from dietary sources. If linoleic acid is not furnished in the diet, signs of deficiency, including growth retardation, skin lesions, and reproductive failure, result. For this reason, linoleic acid is an essential fatty acid (EFA).
Arachidonic acid (18-carbon chain with four double bonds) and linolenic acid (18-carbon chain with three double bonds) are also considered EFAs, but healthy individuals can produce them from sufficient quantities of linoleic acid (see Chapter 2, Fig. 2-13). Linolenic acid can be converted rapidly into omega-3 fatty acids in the body. The conversion of linolenic acid to EPA and the conversion of linoleic acid to arachidonic acid are competitive because the processes use the same enzyme. Studies suggest that less than 10% of linolenic acid is converted to EPA. When intake of linoleic acid is substantially higher than intake of linolenic acid, less EPA is available. Linolenic acid may be a protective factor against CHD (Table 6-1).5
Table 6-1
Common food sources and physiological actions of fatty acids
| Fatty Acid Classification | Common Food Sources | Physiological Action |
| Saturated Fatty Acid (SFA) | ||
| Coconut oil, butter fat, most fats and oils, cocoa butter, fully hydrogenated vegetable oils | Raises total, LDL and HDL cholesterol (except stearic acid) | |
| Monounsaturated Fatty Acid (MUFA) | ||
| Cis configuration | Some fish oils, beef fat, most fats and oils, nuts, seeds, avocados | Decreases total and LDL cholesterol when substituted for SFAs and decreases total cholesterol compared with dietary carbohydrate |
| Trans configuration | Partially hydrogenated vegetable oils | Raises total and LDL cholesterol similar to SFAs, decreases HDL more than saturated fatty acids, and raises total-to-HDL ratio more than SFAs |
| Trans configuration | Dairy fat, meat from ruminating animals (beef, lamb) | May have beneficial health effects, especially vaccenic acid; more research needed |
| Polyunsaturated Fatty Acid (PUFA) | ||
| n-6 Fatty Acids | ||
| Linoleic acid | Liquid vegetable oils, nuts, seeds | Decreases total and LDL cholesterol |
| Arachidonic acid | Meat, poultry, fish, eggs | Precursor for important biologically active substances; substrate for synthesis of a variety of proinflammatory compounds |
| n-3 Fatty Acids | ||
| α-Linolenic acid | Flaxseed, canola oil, soybean oil, walnuts | Decreases cardiovascular risk |
| Eicosapentaenoic acid (EPA) Docosahexaenoic acid (DHA) |
Fish oil, algae | Decreases risk of sudden death from cardiovascular conditions and has beneficial effects on nervous system development and health |
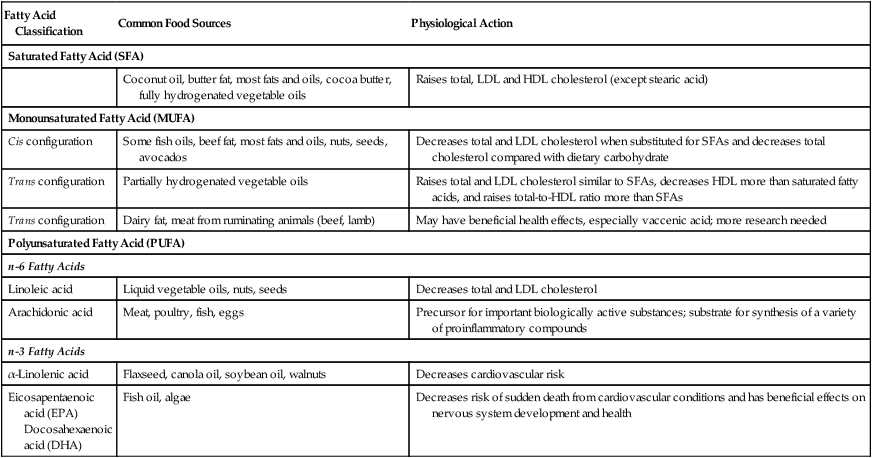
Adapted from Kris-Etherton P, Innis S: Position of the American Dietetic Association and Dietitians of Canada: dietary fatty acids. J Am Diet Assoc 2007; 107(9):1599-1611.
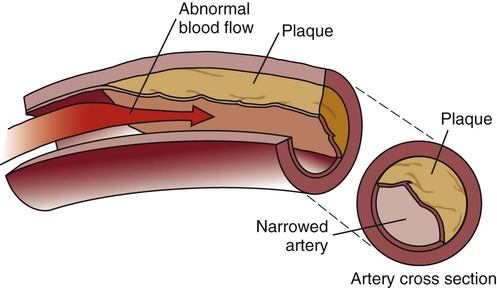
Omega-3 fatty acids are used to produce compounds regulating blood pressure, clotting, immune responses, gastrointestinal secretions, and cardiovascular functions; they also prevent heart arrhythmias and decrease triglyceride levels. Omega-3 fatty acids are essential for the development of brain and retinal tissues in fetal and neonatal development, and ongoing cognitive development in childhood. The presence of omega-3 fatty acids in the diet has been linked to reduction or amelioration of several chronic diseases, including CHD, atherosclerosis and atherosclerotic plaque, and mortality risk from CHD (Fig. 6-5),6 rheumatoid arthritis, psoriasis, inflammatory and immune disorders, and serious eye problems such as macular degeneration (see Table 6-1). However, in numerous studies, supplementation has not been associated with either lower risk of all-cause mortality or major CHD outcomes.7 Studies are exploring the relationship of omega-3 fatty acids with mental aging and Alzheimer disease.
Dietary Fats and Dental Health
1. Some fatty acids, specifically oleic acid, are growth factors for lactic acid bacteria, whereas streptococcal organisms are inhibited by lauric acid (Lauricidin).
2. Long-chain fatty acids may reduce dissolution of hydroxyapatite by acids.
3. Oral food retention is reduced by fat intake.
4. Fats may lubricate the tooth surface and prevent penetration of acid to the enamel (i.e., the “greased” tooth is impervious to acid, protecting caries-susceptible areas).
5. Fats may produce a film on food particles and prevent partial digestion of food particles in the mouth.
6. Dietary fat delays gastric emptying, enhancing fluoride absorption, and increasing tissue fluoride concentration.
Bacterial inflammation and systemic immune response are believed to play a central role in the initiation and propagation of atherosclerosis. Periodontal diseases (including gingivitis and periodontitis) are oral conditions caused by bacteria (and poor oral hygiene) that are risk factors contributing to coronary artery disease. When bacteria are allowed to grow rampantly in the mouth, inflammation may occur throughout the body. Bacteria from dental plaque biofilm can cause blood clots when they escape into the bloodstream and could be involved in inflammation of the lining of blood vessels and atherosclerosis. This inflammation may serve as a base for development of arterial atherosclerotic plaques, but—contrary to some concerns—omega-6 fatty acids do not seem to promote inflammation.8 Research studies show that the inflammatory process can be attenuated by n-3 fatty acids.9 Consumption of greater amounts of docosahexaenoic acid (DHA) and—to a lesser degree—EPA were associated with lower prevalence of periodontitis.10
 Dental Considerations
Dental Considerations
• Although fat intake may have a positive effect on dental health, the medical history of the patient needs to be considered when providing nutrition education.
• Lipids as a source of energy provide 9 kcal/g, whereas carbohydrates and proteins provide 4 kcal/g.
• Fish consumption may have a favorable effect on blood platelets and other blood clotting mechanisms, reducing the risk of clot formation.
• The only proven benefit and suggested use of lecithin supplements is for individuals taking niacin to treat high cholesterol levels because niacin can deplete the body’s stores of choline.
• Interview the patient to evaluate total fat intake. Everyone needs adequate amounts of fat to allow protein to perform its functions of building and repairing. If total energy intake is inadequate, healing is slower. Also, inadequate fat intake could lead to secondary deficiencies of fat-soluble vitamins.
• Foods such as nuts and certain cheeses (cheddar, Monterey Jack, Swiss) may protect teeth against acid attack, especially when consumed after fermentable carbohydrates. Even though they are generally considered nutritious foods, they have a relatively high fat content and may not be appropriate for all people.
• Because omega-3 fatty acids may be beneficial to health, determine the patient’s frequency of fish consumption and supplement use. An increase in fish consumption is recommended for most patients, but some fish, especially mackerel and tuna, should be consumed in moderation because of their mercury content.
• Do not advocate indiscriminate use of omega-3 fatty acid supplements. Although fish oils are beneficial for many conditions, they may have a negative effect on blood glucose levels in patients with diabetes mellitus. If the patient is consuming omega-3 fatty acid supplements, inquire about the quantity. Intakes of more than 3 g should be supervised by a healthcare provider.
• Krill oil (a type of fish oil) contains omega-3 fatty acids, but is more expensive than other omega-3 supplements. Studies have not shown convincing evidence that health benefits of krill oil are superior to those of regular fish oil.
• If the patient is taking anticoagulants or aspirin, evaluate use of omega-3 fatty acids. These patients may be prone to bleeding problems or poor wound healing.
• Structural differences among the various trans fatty acids result in different health effects.
 Nutritional Directions
Nutritional Directions
• Although digestion of fried foods takes longer, the process is as complete as that of other foods in most individuals if food is fried at the proper temperature.
• Fats act as a lubricant in the intestines, decreasing constipation.
• Foods containing trans fats include stick margarine, vegetable shortening, peanut butter, commercially baked goods (cookies, crackers, biscuits, cake, and breads), potato chips, salad dressing, and fast foods (french fries, doughnuts, and other fried foods). Products containing partially hydrogenated (or trans) fats should be limited because trans fats behave like saturated fat in the body.
• Patients should consult their healthcare provider or an RDN before taking an omega-3 fatty acid supplement. Foods containing omega-3 fatty acids should be included in the diet at least 2 times a week to enjoy good health and prevent many diseases.
• Educate patients on how to read labels of omega-3 fatty acid supplements. Supplements made from liver should be avoided because high levels of pesticides or heavy metals may be present.
• The potential relationship between periodontal disease and heart disease emphasizes important health reasons for good dental hygiene.
• Avoid choosing a product containing less trans fats but more saturated fat because both have undesirable effects on blood lipids.
Dietary Requirements
A certain amount of fat is needed to provide adequate amounts of fat-soluble vitamins and EFAs. The acceptable macronutrient distribution range for fat is estimated to be 20% to 35% of energy intake for adults (Table 6-2). The lower limit for fat intake was established to minimize the increase in blood triglyceride levels and decrease in HDL cholesterol levels that occur with higher intakes of carbohydrates. The upper limit of 35% kcal from fat was based on information indicating higher fat intake is associated with a greater intake of energy and SFA, which may be detrimental to health. Box 6-1 shows a method for calculating the IOM recommendation for dietary fat.
Table 6-2
Fat recommendations for adults*
| Classification of Fat | Dietary Guidelines | IOM† Reference Dietary Allowance (RDA)/Adequate Intake‡ (AI) | IOM† Acceptable Macronutrient Distribution Range (AMDR) | American Heart Association§ | American Diabetes Association¶ | Canada’s Food Guide** |
| Total fat | 20% to 35% kcal | — | 20% to 35% kcal | 25% to 35% kcal | — | 20% to 35% kcal |
| Saturated fatty acids (SFA) | <10% kcal | Minimize | Minimize | <7% kcal (stay away from tropical oils such as coconut oil, palm oil and palm kernel oils that are high in SFA) | <7% kcal | Limit butter, hard margarines, lard, and shortening |
| Trans fatty acids (TFA) | <1% kcal | Minimize¶¶ | Minimize¶¶ | >1% kcal | Minimize¶¶ | Limit hard margarines, lard, and shortening |
| Omega-6 fatty acids (n-6 PUFA) | 14 g/day for males; 11 g/day for females | 5% to 10% kcal | Choose monounsaturated fatty acids (MUFA) or PUFA (vegetable oils, margarines with liquid vegetable oil as the first listed ingredient) | Use vegetable oils, such as canola, olive, and soybean | ||
| α-Linolenic acid | 1.6 g/day for males; 1.1 g/day for females | 0.6% to 1.2% kcal | No specific recommendation |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


