Introduction
The emphasis on dental esthetics has increased in recent years. There are, however, differences in esthetic perceptions among professional and lay groups. The aim of this comprehensive review was to update previous reviews and answer the following research question: Can lay thresholds for acceptance of smile esthetic anomalies be defined?
Methods
A systematic search in the medical literature (PubMed, PMC, NLM, Embase, Cochrane Central Register of Controlled Clinical trials, Web of Knowledge, Scopus, Google Scholar, and LILACs) was performed to identify all peer-reviewed articles reporting data regarding evaluations of laypeople’s perceptions of dental esthetic factors.
Results
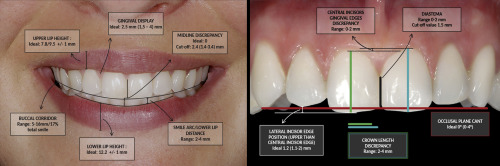
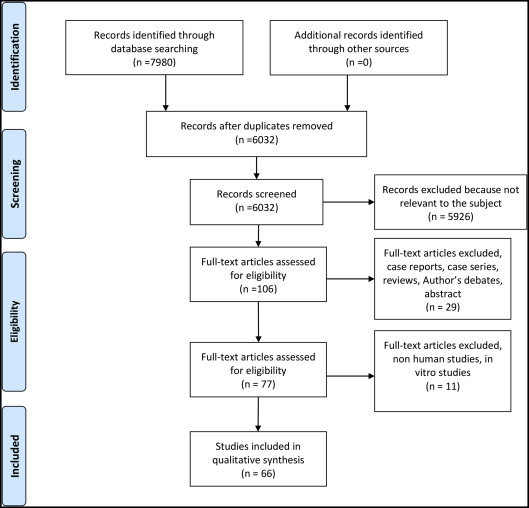
Of the 6032 analyzed articles, 66 studies were selected for the final review process. Among the selected articles investigated perceptions of diastema, 15 analyzed modifications in tooth size and shape, 8 considered incisor positions, 15 evaluated midline discrepancies, 16 investigated buccal corridors, 26 analyzed gingival display and design, 3 considered lip height, and 20 investigated miscellaneous factors. Threshold values were identified for the following features: diastema (0-2 mm), tooth size and shape of incisor position, midline discrepancy (0-3 mm), buccal corridors (5-16 mm), gingival exposure (1.5-4 mm), occlusal canting (0°-4°), and overbite (2-5 mm). Furthermore, few other smile characteristics were found to be significantly associated with perception of smile aesthetics, even though any threshold could be detected.
Conclusions
On the basis of the obtained results, threshold values for the main features of smile and dental esthetics could be identified. Limitations of the present study were the heterogeneity of data which made it impossible to perform a meta-analysis, and the lack of information about sample selection and selective outcome reporting.
Graphical abstract
Highlights
- •
Thresholds for the main features of smile and dental esthetics could be identified.
- •
Overall risk of bias was low to moderate.
- •
This review is the first attempt to quantify laypeople’s smile esthetic perceptions.
The emphasis on dentoalveolar esthetics has increased among both dental professionals and patients in recent years. Moreover, although an ideal occlusion remains a primary goal of treatment, the esthetic outcome is critical for a patient’s satisfaction. Many of those seeking orthodontic treatment are keen to improve dental esthetics and, potentially, their quality of life regarding both functional aspects and appearance.
According to Sarver and Jacobson and Sarver and Ackerman, it may be inappropriate to place everyone in the same esthetic framework and even more problematic to attempt this based solely on hard tissue relationships, since the soft tissues often fail to respond predictably to hard tissue changes. Nevertheless, it is accepted that esthetic considerations are paramount in planning appropriate and orthognathic treatment but that rigid rules cannot be applied to this process. In view of our inability to apply rules defining optimal esthetics, the use of scientific methods to plan the most esthetic treatment may therefore be complicated.
Nevertheless, it is clear that laypeople can identify various factors affecting smile esthetics. Perception is defined as a cognitive process involving interpretation of a stimulus and recognition of the object producing a sensation. This process is based on earlier experience, and it represents the instrument by which one becomes acquainted with the environment. Perception has a psychological basis and therefore is not simply allied with sensation. Commonly, the perceptions of others can produce an environment that might affect a person’s social and intellectual development. It has also variously been confirmed that others’ perceptions can influence the way a person acts and even result in long-term developmental changes and varying levels of achievement. Regarding facial appearance, Goldstein found that the eyes and the mouth were the most important factors in a hierarchy of characteristics for determining esthetic perceptions.
It is accepted that there is often a discord between lay and professional opinions in relation to dental esthetics. Thus, clinicians can expect their patients to be more attentive to some dental esthetic factors than they are to others. Furthermore, it is important to define the thresholds of esthetic acceptability for facial and dental esthetic problems: ie, the minimum level of esthetic harmony that can be approved as pleasurable by an external observer. Thus, the aim of this study was to assess laypeople’s evaluations of adult smile appearance, aiming to identify thresholds of acceptance for esthetic alterations.
Materials and methods
Protocol and registration
This comprehensive review protocol was registered in the International Prospective Register of Systematic Review ( http://www.crd.york.ac.uk/PROSPERO/ ; protocol number CRD42015017781) and modified in January 2016.
Eligibility criteria
The inclusion and exclusion criteria are presented in Table I . The reference lists of included articles were perused, and references related to the articles were followed up.
| Inclusion criteria | Exclusion criteria |
|---|---|
| Randomized and nonrandomized prospective, retrospective, and observational original studies analyzing the perceptions of laypeople about dental and smile esthetics | Studies that investigated only facial esthetics without any dentoalveolar link |
| Studies with adequate statistical analyses | Studies that investigated dental esthetics from a lateral aspect rather than from frontal aspect |
| Studies with an analyzed sample of at least 10 observers | Studies that investigated self-perceptions of esthetics |
| Studies that compared laypeople’s esthetic perspectives with those of another group, without reporting laypeople’s specific opinions | |
| Descriptive studies | |
| Editorials | |
| Letters | |
| Reviews |
Information sources, search strategy, and study selection
On April 1, 2016, a systematic search in the medical literature was performed to identify all peer-reviewed articles reporting data regarding the evaluation of laypeople’s perceptions of dental esthetic factors. To retrieve lists of potential articles to be included in the review, searches of PubMed, PMC, NLM, Embase, Cochrane Central Register of Controlled Clinical trials, Web of Knowledge, Scopus, Google Scholar, and LILACs were performed using the following search strategy: (dent* or tooth or teeth or smil*) AND (esthetic* OR aesthetic*) AND (perception OR perspective OR evaluat* OR awareness OR attention).
The bibliographies of the selected articles were thoroughly analyzed for additional articles. Title and abstract screening was performed by 2 authors (G.R., S.P.) to select articles for full text retrieval. The literature search was performed by these authors. Duplicates were removed, and articles were selected for inclusion independently by the same 2 authors. Disagreements were resolved by discussion among all the authors. The list of articles that narrowly failed to meet the inclusion criteria with the reasons for exclusion, is reported in Appendix A .
Data items and collection
A customized template for data extraction was created according to the review requirements because any standard template (eg, PICOS) did not necessarily apply to all included articles ( Appendix B ). The data extraction form was piloted on a sample of 15 articles before being checked and revised if needed by authors who did not extract the data (G.R., S.P.). To summarize the findings of the review, a synthesis has been provided in Table II according to GRADE criteria. All articles were assessed separately by the investigators (T.C., A.F.); in cases of divergent assessments with regard to the assignment of strengths and weaknesses, consensus was reached by discussion with all authors.
| Outcome | Threshold/ideal value (range of acceptability) | Participants (studies) (n) | Quality of the evidence (GRADE) | Comments |
|---|---|---|---|---|
| Diastema | Cutoff value: 1.5 (0-2) mm | 831 (10) | Moderate | 5 RCTs among 10 articles |
| Tooth size and shape | Crown-length discrepancy range: 2-4 mm | 1706 (17) | Moderate | 6 RCTs among 17 articles. For other features in this group, no threshold was identified |
| Incisor position | Lateral incisors’ edge position (maxillary to the central incisor plane) Ideal value: 1.2 (1, 1-2) mm |
376 (6) | Moderate | 2 RCTs among 6 articles. For other features in this group, no threshold was identified |
| Midline discrepancy | Ideal value: 0 Cutoff value: 2.38 (1.83-2.92) mm |
1916 (15) | Moderate | 5 RCTs among 15 articles |
| Buccal corridors | Ideal value: 11.5 (5-16 mm/17% total smile) | 2613 (16) | Moderate | 3 RCTs among 16 articles |
| Gingival display | Ideal value: 2.5 (1.5-4) mm | 2689 (24) | Moderate | 8 RCTs among 24 articles |
| Lip height | Upper lip: 7.8/9.5 ± 1 mm Lower lip: 12.2 ± 1 mm |
146 (3) | Moderate | 1 RCT among 3 articles |
| Miscellaneous | Occlusal plane cant Ideal value: 0° (0°-4°) |
1817 (17) | Moderate | 5 RCTs among 17 articles. For other features in this group, no threshold was identified |
The outcomes from each study were extracted and categorized as follows: diastema, tooth size and shape, incisor positions, midline discrepancies, buccal corridors, gingival exposure, lip height, and miscellaneous.
Primary outcomes included laypeople’s ratings of attractiveness scores for various dentoalveolar anomalies. The secondary outcome included the thresholds of acceptance identified. Each outcome was assessed from smile or facial photographs that may have been digitally manipulated to outline the esthetic alterations in different ways.
Quality assessment in individual studies
According to the Centre for Reviews and Dissemination at the University of York in the United Kingdom and the PRISMA statements, an evaluation of risk of bias within and across studies was performed by 1 author (A.D.) to determine the level of evidence related to each of them ( Fig ). Scoring systems obtained through consensus conferences, such as Cochrane Tool for Risk of Bias Assessment, are usually adopted for risk of bias assessment. However, the studies analyzed in this review were nonclinical studies; thus, they did not fit any standard tool for methodologic quality analysis. Risk of bias among studies was assessed with a dedicated tool ( Table III ).
| Author, year | Participants (judges) involved in evaluation (n) | Participant source | Presentation type | Viewing protocol | Intraexaminer reliability | Scoring technique | Methodologic score according to Witt and Flores-Mir |
|---|---|---|---|---|---|---|---|
| Abu Alhaija et al, 2011 | 4 | 3 | 4 | 2 | 2 | 3 | 18 |
| An et al, 2009 | 4 | 3 | 4 | 1 | 1 | 1 | 14 |
| An et al, 2014 | 4 | 3 | 5 | 4 | 2 | 3 | 21 |
| Anderson et al, 2005 | 4 | 3 | 4 | 2 | 2 | 3 | 18 |
| Badran and Mustafa, 2013 | 4 | 3 | 4 | 3 | 2 | 3 | 19 |
| Beyer and Lindauer, 1998 | 3 | 2 | 4 | 3 | 2 | 3 | 17 |
| Brough et al, 2010 | 3 | 3 | 6 | 4 | 2 | 1 | 19 |
| Chang et al, 2011 | 4 | 3 | 6 | 2 | 1 | 3 | 19 |
| Correa et al, 2014 | 3 | 2 | 6 | 2 | 1 | 3 | 17 |
| De-Marchi et al, 2012 | 2 | 2 | 4 | 4 | 2 | 3 | 17 |
| Farzanegan et al, 2013 | 2 | 1 | 4 | 3 | 2 | 3 | 15 |
| Feu et al, 2011 | 3 | 1 | 4 | 1 | 2 | 1 | 12 |
| Geron and Atalia, 2005 | 4 | 3 | 4 | 2 | 2 | 3 | 18 |
| Gracco et al, 2006 | 4 | 1 | 4 | 2 | 1 | 2 | 14 |
| Guo et al, 2013 | 4 | 2 | 6 | 4 | 1 | 2 | 19 |
| Ioi et al, 2012 | 4 | 1 | 5 | 1 | 2 | 3 | 16 |
| Ioi et al, 2014 | 4 | 2 | 4 | 1 | 2 | 3 | 16 |
| Johnston et al, 1999 | 2 | 2 | 6 | 1 | 2 | 3 | 16 |
| Ker et al, 2008 | 4 | 3 | 4 | 2 | 2 | 3 | 18 |
| Kim and Gianelly, 2003 | 3 | 1 | 4 | 1 | 2 | 2 | 13 |
| Kaya and Uyar, 2013 | 3 | 1 | 5 | 1 | 2 | 3 | 15 |
| Kaya and Uyar, 2016 | 3 | 1 | 4 | 4 | 2 | 3 | 17 |
| King et al, 2008 | 3 | 1 | 5 | 4 | 2 | 2 | 17 |
| Kokich et al, 1999 | 4 | 1 | 4 | 1 | 2 | 3 | 15 |
| Kokich et al, 2006 | 4 | 1 | 4 | 1 | 2 | 3 | 15 |
| Kumar et al, 2012 | 3 | 2 | 4 | 1 | 2 | 3 | 15 |
| LaVacca et al, 2005 | 3 | 2 | 5 | 4 | 2 | 3 | 19 |
| Ma et al, 2014 | 4 | 1 | 4 | 1 | 2 | 3 | 15 |
| Machado et al, 2013 | 4 | 2 | 6 | 4 | 1 | 2 | 19 |
| Machado et al, 2013 | 3 | 1 | 5 | 2 | 2 | 3 | 15 |
| Machado et al, 2013 | 3 | 1 | 5 | 2 | 2 | 3 | 15 |
| Martin et al, 2007 | 3 | 3 | 4 | 2 | 2 | 3 | 17 |
| McLeod et al, 2011 | 4 | 3 | 4 | 1 | 2 | 3 | 17 |
| McNamara et al, 2008 | 3 | 1 | 4 | 2 | 1 | 3 | 14 |
| Moore et al, 2005 | 3 | 1 | 6 | 4 | 2 | 3 | 19 |
| Musskopf et al, 2013 | 3 | 2 | 4 | 4 | 2 | 3 | 18 |
| Nascimento et al, 2012 | 3 | 1 | 4 | 2 | 1 | 3 | 14 |
| Noureddine et al, 2014 | 3 | 1 | 6 | 4 | 2 | 3 | 19 |
| Olivares et al, 2013 | 3 | 1 | 4 | 4 | 2 | 3 | 17 |
| Ong et al, 2006 | 2 | 1 | 4 | 3 | 2 | 3 | 15 |
| Parekh et al, 2006 | 4 | 3 | 5 | 4 | 2 | 3 | 21 |
| Parekh et al, 2007 | 4 | 3 | 5 | 1 | 2 | 3 | 18 |
| Pinho et al, 2007 | 3 | 1 | 4 | 3 | 2 | 3 | 16 |
| Pithon et al, 2012 | 4 | 1 | 4 | 2 | 2 | 3 | 16 |
| Pithon et al, 2012 | 3 | 1 | 4 | 4 | 2 | 3 | 17 |
| Pithon et al, 2012 | 3 | 1 | 4 | 4 | 2 | 3 | 17 |
| Pithon et al, 2013 | 3 | 1 | 5 | 4 | 2 | 3 | 18 |
| Pithon et al, 2015 | 4 | 1 | 4 | 2 | 2 | 3 | 16 |
| Roden-Johnson et al, 2005 | 2 | 1 | 5 | 1 | 1 | 3 | 13 |
| Rodrigues et al, 2009 | 2 | 2 | 4 | 3 | 2 | 3 | 16 |
| Rodriguez-Martinez et al, 2013 | 3 | 1 | 5 | 3 | 2 | 3 | 16 |
| Rosa et al, 2013 | 3 | 1 | 3 | 2 | 2 | 3 | 14 |
| Saunders et al, 2011 | 3 | 3 | 6 | 2 | 2 | 3 | 19 |
| Silva et al, 2013 | 2 | 1 | 4 | 3 | 2 | 3 | 15 |
| Springer et al, 2011 | 3 | 3 | 6 | 2 | 2 | 3 | 19 |
| Suzuki et al, 2009 | 2 | 1 | 4 | 1 | 2 | 3 | 13 |
| Talic et al, 2013 | 3 | 1 | 4 | 1 | 2 | 3 | 13 |
| Thomas et al, 2003 | 3 | 2 | 6 | 4 | 2 | 3 | 20 |
| Thomas et al, 2011 | 4 | 1 | 5 | 2 | 2 | 3 | 17 |
| Williams et al, 2014 | 4 | 3 | 6 | 4 | 2 | 3 | 22 |
| Wolfart et al, 2004 | 3 | 2 | 3 | 3 | 1 | 3 | 15 |
| Xu et al, 2015 | 3 | 2 | 3 | 4 | 2 | 3 | 17 |
| Yang et al, 2015 | 3 | 1 | 6 | 4 | 2 | 3 | 19 |
| Zange et al, 2011 | 3 | 1 | 4 | 4 | 2 | 3 | 13 |
| Zhang et al, 2010 | 4 | 2 | 6 | 4 | 2 | 3 | 21 |
| Zhang et al, 2016 | 3 | 2 | 6 | 3 | 2 | 3 | 19 |
Summary measures and approach to synthesis
Clinical heterogeneity of the included studies was evaluated by assessing the participants and settings, index tests, and measurement techniques. For accuracy of measurements, mean differences, with measures of dispersion, were reported where available.
Results
Study selection and characteristics
Among the 6032 analyzed articles, 66 were selected for the final review process. The article selection procedure have been described in the PRISMA flow chart ( Fig ). Among the selected articles, 10 investigated perceptions of diastema, 15 analyzed modifications in tooth size and shape, 8 considered incisor positions, 15 evaluated midline discrepancies, 16 investigated buccal corridors, 26 analyzed gingival display and design, and 3 considered lip height; in 20, miscellaneous factors were investigated. The overall number of recruited evaluators was 7088 (2887 female, 2123 male, and 2078 unspecified; range, 20-1275 per study). Mean ages of the subjects in the evaluated samples ranged from 12 to 74 years. A visual analog scale (VAS) was adopted in 34 studies, a Likert-type scale was used in 7 studies, 16 used generic point scales, 3 adopted surveys or questionnaires, 1 study used VAS and a separate questionnaire, 3 evaluated only the minimum and maximum values, and 2 studies used rank ordering.
Quality within studies
According to the criteria, the overall mean score of quality of studies was 16.8 of a possible 22. The highest score assigned to an article was 22 points, and the lowest score assigned was 13 points.
Results of individual studies, meta-analysis, and additional analyses
A meta-analysis of the results of the studies was planned. However, because of the high degrees of clinical heterogeneity and variations in terms of sampling and outcome analysis, meta-analysis was not possible. Results from individual studies were therefore assessed, and estimates of esthetic thresholds have been suggested. Further research is warranted to confirm these.
Diastema
Ten articles analyzed diastema perception, and only 3 provided information on a threshold of acceptance. Kokich et al identified a threshold of 2 mm for diastema. Kumar et al stated a threshold of 1.5 mm. Machado et al reported that for both extraction and nonextraction patients, the most attractive smile had no spacing, whereas the greater and the more mesially located was the diastema, the more unattractive the smile. Noureddine et al stated that the width of the midline diastema has a significant impact on smile esthetics, even when associated with lateral spaces. Abu Alhaija et al assumed a cutoff as low as 1 mm, although they observed that female judges were more tolerant (3-mm threshold). Based on these studies, an overall mean esthetic cutoff about 1.5 mm may be reasonable.
Tooth size and shape
Fifteen articles evaluated discrepancies in tooth dimensions and shape. Anderson et al stated that square or round incisors were more attractive for masculine smiles, and that incisor shape was instrumental in anterior dental esthetics. Only 1 study focused on canine esthetics, reporting that increased canine tip height and pointed canines were perceived to be unattractive. Five articles established a threshold of attractiveness for crown-length discrepancy, which ranged between 2 and 4 mm.
Tooth position
Eight articles investigated tooth position. Machado et al, based on judgments of an ethnic sample, showed that smiles with a maximum of 0.5 mm of asymmetry on the lateral incisors were considered attractive. Furthermore, 0.5 mm of wear of the central incisor was considered extremely unattractive. These findings were corroborated by Ma et al, who observed that discrepancies related to central incisors had a much greater impact on smile esthetics than lateral incisors. Moreover, Rodrigues et al showed that a lateral incisor distal inclination of 10° did not affect smile esthetics. Regarding tooth position, the literature supports a threshold by laypeople only for lateral incisor edge position, corresponding to a range between 1.1 and 2 mm superior to the level of the central incisors, whereas the ideal position was calculated as 1.2 mm. Furthermore, Chang et al showed different ideal values for female (1.2 mm) and male (2.0 mm) subjects.
Midline discrepancy
Fifteen articles analyzed the perceptions of midline discrepancy. Seven of them established a mean threshold of acceptance for midline deviations (2.1 mm, 2 mm, 2.92 ± 1.1 mm, 263 mm, 1.83 mm, 2.40 mm, and 2.6 mm ), and Kokich et al and Pinho et al could not identify a reference value. An overall mean acceptable value of 2.38 mm was calculated from the sample. The minimum detected threshold was 1.83 mm, whereas the maximum accepted one was 2.92 mm. However, Rodrigues et al found no differences in the perceptions of an ideal smile and a midline deviation of 3 mm, highlighting the variability in perceptions. Regarding midline inclination, Thomas et al proposed a tolerance level of 10° ± 6° of angulation.
Buccal corridors
Sixteen articles evaluated the impact of buccal corridors on smile esthetics.
Moore et al observed that the best rated amount of buccal corridors was 2% of the smile area. Three articles stated a threshold value for acceptability of the amount of buccal corridors (17% ; minimum 5.5 mm or 8%, maximum 16 mm or 22% ; minimum 5.07 mm and maximum 14, 25 mm ). Furthermore, the range of tolerance varied from 5 to 16 mm, but when calculated as a ratio of the smile area, a maximum of 17% was identified. The ideal size of the buccal corridors was therefore discordant, with McLeod et al alluding to a 6-mm optimum value, and Ker et al identified an optimum value of 11.6 mm with an ideal percentage of 16%. Zange et al highlighted a threshold of 28% of buccal corridors in patients with long face and short face patterns, with short face patterns receiving better scores. Abu Alahjia et al and Badran and Mustafa showed that laypeople preferred minimal or no buccal corridors even if the buccal corridors did not affect significantly smile esthetics, as confirmed by Roden-Johnson et al. Parekh et al observed that flat smile arcs increased the impact of buccal corridors on esthetics. Clearly, there appears to be little consistency for the preferred levels of buccal corridors.
Gingival display and design
Perceptions of gingival display and gingival design or height were analyzed in 26 articles. Eleven articles stated a threshold of acceptance for gingival exposure (4 mm ; 3 mm ; Likert scale, 1 mm: 1.80/5, 4 mm: 2.36/525; VAS, unaltered, 5.85/10, 4 mm: 5.7/10 ; VAS, 0 mm: 63.1/100, 5 mm: 54.3/100 ; VAS, 0 mm: 64.92/100, 2 mm: 21.89/100 ; minimum, 0.8 mm, maximum 4.5 mm ; minimum, 4.0 mm, maximum, −3.6 mm ; minimum, 2.7 mm, maximum, −2.52 mm ; VAS, 0 mm: 41.5/100, 2.5 mm: 20.9/100 ; −1 mm ), and 2 articles identified an ideal value (2.1 mm, and 2.7 mm ). Kaya and Uyar and Suzuki et al stated that a gingival display of 2 mm or more negatively affects esthetics. Geron and Atalia highlighted 1 mm of exposure for the maxillary arch and 0 mm for the mandibular arch as thresholds of acceptability; thus, scores decreased with increasing gingival display, as confirmed by Pithon et al.
Regarding gingival design, Musskopf et al highlighted a 2-mm threshold for gingival recession. Brough et al assumed that canine gingival height 0.5 mm below the gingival margin of the maxillary central incisor was the most attractive.
Correa et al and Ker et al showed that a discrepancy of 2 mm for maxillary central incisor gingival height and a discrepancy of 1.2 mm for maxillary lateral incisor gingival height were significantly correlated with a worse smile evaluation. Feu et al noticed that asymmetries of incisal gingival height discrepancy greater than 2 mm were perceived by laypeople.
Lip height
Three articles evaluated the impact of lip height on smile scores. In a Japanese and Korean sample, a range of attractiveness of −1 to +1 mm for the average vermilion height was proposed by Ioi et al. However, lip thickness and lower lip to maxillary incisor distance appeared to influence significantly the overall esthetic smile scores.
Miscellaneous
Miscellaneous factors that may affect perceptions of esthetic were analyzed in 20 articles. Seven articles concluded that the smile arc influences esthetic attractiveness. Parekh et al found flat smile arcs to be extremely objectionable, but it appears that some increments flatter than ideal are acceptable. Ker et al found that more upward curvature beyond what follows the lower lip did not rate well. Springer et al identified a threshold of 4 mm for the distance between the smile arc and the lower lip (ideal value, 2 mm), whereas Badran and Mustafa highlighted that a reverse smile arc has a negative effect on esthetic perceptions, considerably worse for orthodontists than for laypeople. Kim and Gianelly stated that constricted arch widths are not a usual outcome of extraction treatment and that neither extraction nor nonextraction treatment has a preferential effect on smile esthetics. Four articles analyzed the importance of occlusal canting, with a threshold value of 4° identified and an ideal value of 0°. Olivares et al reported a significantly greater awareness of these defects among professionals when compared with laypeople.
Three articles indicated a threshold for overbite acceptance of 5 mm, with an ideal value of 2 mm.
According to Farzanegan et al, the role of the teeth seemed more important than that of the lips in making an esthetic smile, with orthodontists more critical than laypeople. Pinho et al stated that wear of the canine cusps had no esthetic impact. Thomas et al found the symmetry of papillary height to be important for attractiveness. Zhang et al reported that the arch width as observed during a smile from a frontal point of view had a range of acceptability between 31.5 and 38.5 mm. Pithon et al stated that the lowest scores for maxillary anterior tooth exposure during smiling were assigned to the least incisor display (7 mm). Two articles analyzed smile attractiveness after mandibular incisor extractions, reporting a significant negative effect on dental esthetics and significantly lower scores among orthodontists. Xu et al identified a broad esthetic acceptability range for buccolingual inclinations of the maxillary canines and premolars in the frontal view of a smile from 3° to −10° for the canines and 5° to −11° for the premolars.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


