• Figure 14-1 Low-level laser therapy using athermal diode laser.
Safety and Anesthesia Considerations
Although the use of lasers for OMS offers many advantages, it does present certain anesthetic risks not common to traditional surgical techniques. Standard safety precautions must be observed to maintain the safety of the patient, surgeon, anesthesiologist, and other members of the surgical staff. Each laser system’s user manual should be reviewed before initiation of a planned procedure. Also, discussion with the anesthesiologist regarding the type of laser and the procedure is imperative. It is important to be just as vigilant when laser surgery is performed in the outpatient office environment.
The laser beam is a high-intensity light that, if directed at a reflective surface, can change its intended path while maintaining its focal properties. When reflected in this manner, the beam can strike unintended targets with full power. Most vulnerable to injury from a misdirected beam are the eyes, the skin, and any nearby flammable objects.12 Appropriate warning signs should be posted outside the operating suite indicating the type of laser being used, the risk class of the laser, and the required personal safety equipment13 (Figure 14-3). Protective eyewear with eye shields must be worn at all times by the patient and personnel to avoid ophthalmic injury. For each laser, a specific type of eyewear is available that will absorb its particular wavelength.
Flammable patient drapes, including standard paper and plastic drapes used in the operating room (OR), are a source of ignition and should not be used. Instead, laser-resistant drapes or cloth drapes saturated in water should be used around the surgical field.13 Alcohol preparation of the field also should be avoided, because alcohol can serve as a potential ignition source if not allowed to vaporize completely before laser use.

• Figure 14-2 Intense pulsed light (IPL) source. These devices most often are used for vascular and pigmented lesion removal or hair removal. Anesthesia usually is not required for these procedures.
Three main approaches are recognized to decrease the fire hazards associated with use of conventional endotracheal (ET) tubes during laser surgery14: (1) no airway, (2) protection of the surface of a conventional tube, and (3) use of a noncombustible tube. With many OMS procedures, whether done in the office or the operating suite, a total intravenous anesthesia technique may be appropriate after “chinning” the patient (i.e., applying the chin thrust maneuver as for cardiopulmonary resuscitation [CPR]) or insertion of a nasal airway. The Rousch red-rubber nasal airway has been found to be safe for laser procedures.15
The no-airway approach, however, is not always practical for procedures of long duration, in which case a definitive airway, with shielding from the laser beam, is necessary, such as a conventional ET tube with a protective material on its external surface. Materials available for this purpose are metallic foil wrapped around the tube and a silver anode sheet that adheres to the tube.13 The foil often is cumbersome and vulnerable to dislodgement, so that intraoperative manipulation can result in exposure of the tube, whereas the adherence of the silver anode sheet is less likely to lead to exposure.
• Figure 14-3 Warning sign posted outside operating room indicating type of laser being used, class of laser, and required personal safety equipment.

Two types of noncombustible ET tubes are currently available: the metallic tube, which contains no combustible material, and the ceramic-coated tube (Xomed, Inc., Jacksonville, Florida)13 (Figure 14-4). The metallic tube, however, cannot be used for nasal intubation and does not come with a cuff, which prevents the use of a normal anesthesia circuit.
Still other issues warrant consideration in reduction of laser-related fire hazard: Flammable gases must be avoided during laser surgery. Most inhalational anesthetics used in ORs today are not flammable and include sevoflurane, isoflurane, enflurane, and halothane. Ether and cyclopropane, which are no longer used by most anesthesiologists, are combustible and should not be used.13
The concentration of oxygen with inhalational agents also should be addressed. Ideally, the lowest concentration possible is used while maintaining an acceptable oxygen saturation level. To accomplish this aim, the oxygen is diluted with regular compressed air or with helium, both of which reduce flammability (Figure 14-5). Nitrous oxide mixed with oxygen, however, possesses the same flammability as that of oxygen alone and is avoided.12

Tumor-Resective Surgery: Excision versus Ablation
The laser is a versatile surgical instrument that can be used in three basic ways: excision/incision, ablation/vaporization, and hemostasis/coagulation.16 The technique used is based on the clinical situation and three parameters controlled by the surgeon: power, spot size, and time.
Excision
When used for excisional purposes, the laser is basically a “light scalpel” producing precision cuts without the bleeding of traditional scalpel surgery. For optimal results, the spot size should be kept as small as possible with the particular laser used (usually 0.1 to 0.5 mm), which is accomplished by keeping the handpiece at its focal length from the tissue.17 This is known as the focused mode. The focal length is also variable depending on the handpiece, ranging from 1 mm to 1 cm from the end of the handpiece to the tissue.
The technique for excision of a lesion remains the same regardless of the laser system used. It is recommended first to outline the intended incision line by means of the laser beam set at a lower power in an intermittent, gated, or pulsed mode. This mapping will provide superficial guide marks while avoiding deep penetration into the tissue, allowing the surgeon to adjust the location of the margins, if necessary. Of note, for performing an excisional biopsy, an additional 0.5 mm should be added circumferentially to the margin to account for the lateral zone of thermal necrosis associated with the laser.13
After satisfactory outlining has been performed, the laser is switched to continuous-wave mode, and the dots are connected to create the incision. Multiple passes may be required to achieve the desired depth.
Observing the effect of the laser on the tissue during the first pass will allow the surgeon to adjust the parameters of the laser during subsequent passes, if necessary, to achieve the preferred cut. For example, if the depth of the cut is too shallow, the power may be increased or the handpiece moved at slower rate to increase time of exposure. Increasing the power usually is the better option because increasing the time will allow more time for lateral conduction and subsequent lateral thermal damage. On the other hand, if the initial cut is too deep, the power may be lowered or the handpiece moved more quickly, both of which are good options.
After adequate depth of the outlining incision has been achieved, excision of the lesion can begin. This is accomplished by lightly grasping the tissue with a forceps, applying slight traction, and horizontally undermining the lesion while maintaining the laser tip at the focal length. Hemostasis at the surgical site will be excellent, and closure is rarely needed. The exception is the case in which allowing the wound to granulate would give unacceptable cosmetic results.
Ablation
Another common technique carried out with the laser is tissue ablation (also called vaporization). Ablation is used for superficial tissue removal when standard excision would lead to more extensive sectioning than necessary. The targeted lesion usually is confined to the epithelium and underlying submucosa. The advantages of this technique are less scarring, less dysfunction, and less potential for damage to important adjacent structures.
The technique for ablation begins with the same outlining procedure described for the excisional technique. Next, the laser is defocused by moving the handpiece farther from the tissue, thereby widening the laser beam and increasing the spot size. Spot sizes ranging from 1.5 to 3.0 mm typically are used. The now-defocused beam is passed over the lesion in multiple side-by-side strokes, creating multiple U patterns (Figure 14-6).
After the first pass is complete, the depth of penetration is evaluated. If the cut is too shallow, it can be deepened by increasing the power, increasing the time by moving the handpiece more slowly, or decreasing spot size. Increasing the power is the best alternative, whereas increasing time is to be avoided for reasons previously mentioned. Decreasing the spot size is a viable option but will increase the number of strokes required to cover the area.
Conversely, to decrease the depth of penetration, the surgeon can decrease the power, decrease the time by moving the handpiece more quickly, or widen the spot size. Of these, the latter two are the preferred options.
Ablation alone does not allow a biopsy of the lesion to be taken; therefore, if the clinical findings are suggestive of a malignancy or premalignancy, incisional biopsy should be performed before ablation. If the lesion is histologically benign, the surgeon may safely proceed with ablation. If it is malignant, however, wide laser excision is indicated.

Premalignant Lesions
Premalignant lesions may take the form of leukoplakia, erythroplakia, or a mixed form of the two known as erythroleukoplakia. The possibility of malignant transformation of these lesions is 36.3% to 43.0% in the presence of epithelial dysplasia, and 23.4% to 38.0% without epithelial dysplasia.18 Also, patients with these conditions have a 50- to 60-fold greater risk of developing oral cancer than patients without the lesions. Traditional treatment has involved surgical excision with a scalpel, which has many disadvantages compared with laser excision or ablation procedures. The advantages of using a laser include better control of bleeding, less surgical time, more precise tissue removal, less morbidity and complications, and excellent healing with virtually no scarring.19 Many surgeons also believe that the cauterization effect of the laser on blood vessels and lymphatic channels decreases the amount of hematogenous and lymphatic seeding, thereby lowering recurrence rates.20,21
Laser treatment of premalignant lesions is through excision or ablation. Both procedures begin with outlining the lesion, as discussed earlier, with the depth of the cut being deep to the lesion itself, usually 4 to 9 mm.22 If excision is to be performed, the affected tissue is elevated at one end and undermined, with the laser acting as a cutting tool. If ablation is chosen (usually the treatment of choice), the laser is defocused and the tissue removed in the multiple side-by-side U pattern described earlier.
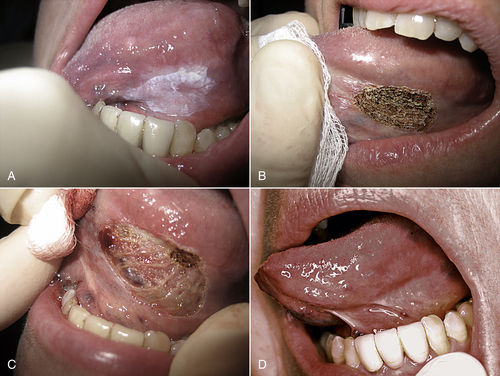
Figure 14-7 illustrates ablation of a leukoplakia on the ventrolateral surface of the tongue. Multiple passes usually are required until removal is complete. With the bloodless surgical field produced by the laser, visual confirmation of complete removal is much easier than during scalpel surgery. The area is then left to reepithelialize by secondary intention, avoiding sutures and the possible distortion and scarring.
Roodenburg et al.18 conducted follow-up evaluations in 70 patients with 103 oral leukoplakias treated with laser ablation at a mean of 5.3 years postoperatively and found a cure rate of 90%. Similarly, Thompson and Wylie23 reviewed the outcomes for 57 consecutive patients with laser-treated oral dysplastic lesions. After 44 months, 76% of the patients exhibited no recurrence. These results are comparable to the 80% success rate seen with conventional scalpel surgery. It is clear that ablation of premalignant lesions is somewhat controversial, although recent evidence indicates that laser ablation is an effective tool for the treatment of this disease process so long as the practitioner remains aware of the risk of recurrence and progression to malignancy.24
Malignant Lesions and Aggressive Benign Lesions
The laser is an accepted and useful surgical tool for the treatment of malignant and aggressive benign lesions of the larynx, pharynx, oral cavity, and lips. Its use offers many advantages not seen with conventional scalpel surgery. Aside from the bloodless surgical field, shorter surgical time, and decreased patient morbidity, advantages specific to these potentially lethal conditions have been recognized. First, lasers seal lymphatic vessels at the surgical margins, which reduces seeding of malignant cells and potential metastasis.25 Second, more nondiseased tissue adjacent to the lesion is preserved. Typical cancer margins are 1.5 to 2 cm beyond any visible or palpable tumor.13 Better visualization, with a bloodless field, allows the surgeon to remove tissue more precisely without sacrificing unnecessary tissue.
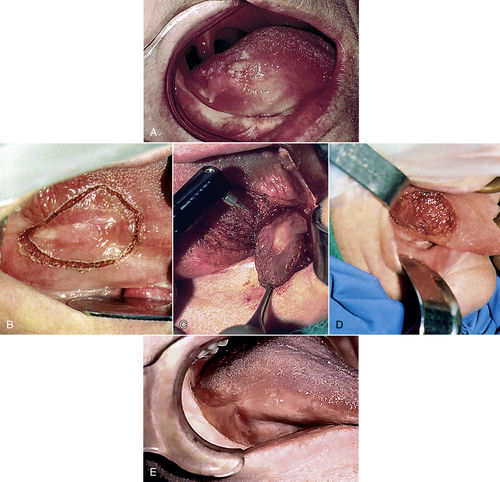
Figure 14-8 demonstrates excision of a T1N0M0 squamous cell carcinoma of the tongue. Laser microsurgery using a surgical microscope helps the surgeon to distinguish between healthy and tumor tissue and to preserve even more normal tissue by taking narrower margins.26 In the event of local tumor recurrence, more retreatment options are available than with conventional scalpel surgery.27
Verrucous carcinoma is a slow-growing, nonmetastasizing form of squamous cell carcinoma that most frequently is found in (but not limited to) the mouth.28 Clinically, this white, cauliflower-like lesion is seen most often in elderly patients.29 The etiology is unknown, but heavy use of tobacco (snuff, chewing tobacco, or cigarettes) may be the primary pathogenetic factor.30,31 Some investigators postulate that human papillomavirus is associated with verrucous carcinoma, but most studies have failed to prove this correlation.32,33 Treatment of these lesions traditionally has been with shave excision, cryosurgery, chemotherapy, or a combination, often necessitating multiple treatments that may lead to scarring.34–36 The CO2 laser has proved to be effective in treating verrucous carcinoma by total excision in cutting mode. Vaporization can be performed on the premalignant form, proliferative verrucous leukoplakia.13
Vascular Lesions
Vascular lesions of the head and neck region are common in patients of all ages. These lesions traditionally are classified as acquired or congenital. Common acquired lesions include telangiectasias, spider and cherry angiomas, pyogenic granulomas, and venous lakes. Vascular lesions are characterized by varying degrees of blood vessel dilation.37 Congenital vascular lesions manifest as either hemangiomas or true vascular malformations.37,38 Histologically, hemangiomas show endothelial cell hyperplasia, whereas vascular malformations are characterized by normal endothelial cells with vessel dilation.39 Hemangiomas are the most common soft tissue tumors of infancy (affecting 5% to 10% of 1-year-olds).40 Traditionally, hemangiomas spontaneously involute between ages 5 and 10 years.41 The most common vascular malformations are port-wine stains, which are present at birth (in 0.3% to 0.5% of the general population42) and do not spontaneously involute.37
The ultimate goal of laser treatment of vascular lesions is selective destruction of abnormal vessels by heating of the vessel wall through the absorption of light by hemoglobin.37 The wavelength chosen should be selectively absorbed by hemoglobin, and the pulse length should be short enough to confine heat to the blood vessels to prevent unwanted damage to adjacent tissue.10 The most common types used for removal of vascular lesions are the KTP, Nd:YAG, and pulsed dye laser (PDL). In addition, IPL systems also may be used.
Telangiectasias are permanently dilated superficial vessels resulting in blue or reddish skin.43 These common asymptomatic lesions often are a cosmetic nuisance to the affected patient. The most common devices used to treat telangiectasias are the PDL and the IPL system. The PDL emits wavelengths of 585 to 600 nm and is better suited for more focal cutaneous lesions; the IPL source emits light in the range of 500 to 1200 nm and is better suited for treatment of more diffuse telangiectasias, such as with rosacea.37 The major drawback of the PDL versus the IPL system is the postoperative purpura, lasting 7 to 10 days.10 The patient should be thoroughly prepared for this preoperatively, and makeup can be applied immediately after the procedure.37
Treatment of port-wine stains is similar to that for telangiectasias because both represent lesions of dilated superficial blood vessels. Port-wine stains typically occur in younger children and can have significant psychological effects during the child’s development if left untreated. The PDL most often is used for eradication of these lesions.40 Multiple treatments usually are required, and lesions partially resistant to the PDL may develop. Pence et al.44 used the frequency-doubled Nd:YAG laser (with a wavelength of 532 nm) to treat 89 patients with port-wine stains of the head and neck for 1 to 12 sessions, with no treatment failures and a rate of adverse side effects (e.g., transient hyper/hypopigmentation, hypotrophic scarring) of 1% to 2%. Therefore combination therapy, with the PDL initially and then the Nd:YAG laser for deeper, more resistant lesions, is likely to produce the best results.
Superficial hemangiomas appear flat and red, whereas deeper lesions appear blue.10 All hemangiomas eventually involute, but delaying treatment can leave lasting cosmetic and psychological scars. Laser treatment of hemangiomas on the skin is similar to that for port-wine stains. The PDL typically is used for hemangiomas with a superficial presentation, whereas the Nd:YAG laser provides the best results for deeper lesions.45 The PDL and the Nd:YAG laser may be used in combination for hemangiomas with superficial and deep components.40
Although most hemangiomas have a cutaneous presentation, these lesions also can occur inside the mouth. Treatment of these intraoral forms is with vaporization or excision, depending on the size of the lesion and its proximity to important neural, vascular, and salivary structures.46 The likelihood of damage to adjacent structures is remote if controlled vaporization is used rather than excision.13 However, hemangiomas that manifest on the tongue, lip, or other areas isolated from important structures can be excised with the CO2 laser. The feeding peripheral vasculature is sealed, and excision can proceed starting with outlining the margins and undermining the lesion, as described earlier.46
It is beyond the scope of this chapter to review all vascular lesions encountered by the oral-maxillofacial surgeon and the associated laser surgery. The interested reader is encouraged to research current trends in the dynamic field of laser surgery for the treatment of these lesions.
Snoring and Sleep Apnea
Laser-Assisted Uvulopalatopharyngoplasty
Snoring is a common social problem, affecting approximately 20% to 30% of the adult population, and has been associated with morning fatigue, restless sleep, daytime somnolence, and hypoxemia.47 In addition to the social implications, snoring can be a risk factor for hypertension, angina pectoris, cerebral infarction, pulmonary hypertension, and congestive heart failure. A significant percentage of snorers also have associated obstructive sleep apnea syndrome (OSAS), marked by repeated episodes of apnea and hypopnea during sleep secondary to collapse of the upper airway despite respiratory effort. Serious medical consequences of OSAS include cardiac arrhythmias, myocardial infarction, systemic and pulmonary hypertension, and increased risk for involvement in motor vehicle crashes.
Although the most common treatment for patients with these sleep-disordered breathing problems has been scalpel uvulopalalatopharyngoplasty (UPPP), this procedure is fraught with complications, including severe pain, hemorrhage, transient nasal regurgitation, permanent velopharyngeal insufficiency, and nasopharyngeal stenosis.48
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


