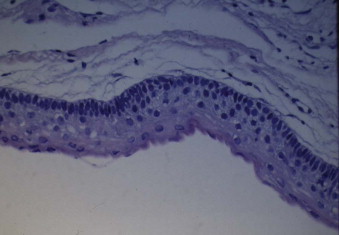
A keratocystic odontogenic tumor (KOT) (formerly known as an odontogenic keratocyst) is a benign cystic tumor of dental origin that probably arises from primitive dental lamina, most commonly occurs in the posterior mandible, and almost certainly represents the lesion that used to be known as a primordial cyst. It has a typical histologic appearance consisting of parakeratinization, a tumor lining five to six cells thick, and polarization of the basal layer on the basement membrane ( Fig. 48-1 ). A KOT is thought to be benign, but locally aggressive. An orthokeratinized version also occurs, but this is thought to represent a different lesion and not to be aggressive. The parakeratinized version is normally quoted as having a recurrence rate varying from 25% to 60% following conservative management such as cystectomy or enucleation. For this reason, alternative treatments have been actively pursued to decrease the recurrence rate but, at the same time, to not subject the patient to radical surgery with loss of teeth, bone, and nerves. The reason for recurrence of KOTs is uncertain. Some authorities believe that they are inherently more aggressive and have a higher mitotic index in the cyst lining, others think that the lining is so friable that it is difficult not to leave small portions behind, and still others believe that it is the presence of epithelial buds or daughter cysts projecting from the lesion that leads to recurrence. Alternative treatments that fall between cystectomy and radical resection are discussed in the following sections.
Decompression or Marsupialization
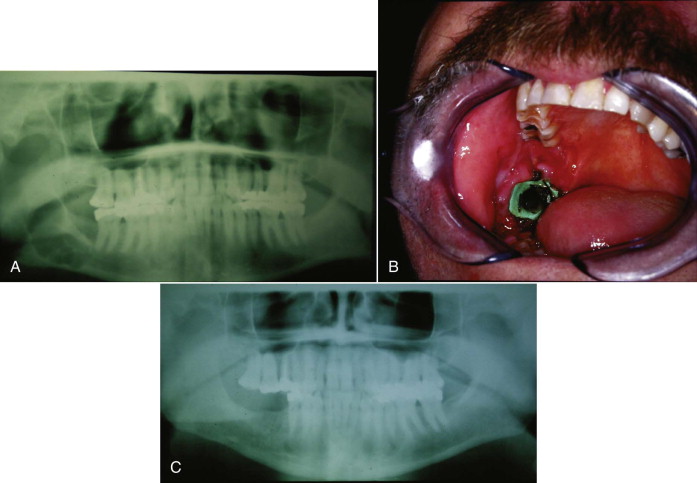
Although these terms are used interchangeably, decompression technically denotes any treatment whereby the pressure is taken off the tumor by creation of a hole in the tumor from which it can drain. This can be a small opening into which a decompression tube can be placed ( Fig. 48-2 ). Decompression is normally used as a means of decreasing the size of a KOT so that it can be enucleated later without risking additional teeth, the inferior alveolar nerve, or the integrity of the mandible.

Marsupialization is a form of decompression that denotes the creation of a wider opening, which is often self-sustaining ( Fig. 48-3 ), and this treatment can be performed for complete cure of the lesion. Although KOT is an aggressive tumor, it does appear to respond successfully to marsupialization and can resolve totally following marsupialization, often over a period of 6 to 12 months ( Fig. 48-4 ). Persistence and recurrences do occur, however, possibly from daughter cysts around the lining, and a personal report shows a 10% recurrence rate with marsupialization alone. Histologic examination has shown that as the marsupialized tumor decreases in size, the lining differentiates from the typical appearance of a KOT to one more closely resembling oral mucosa. Whether this occurs by metaplasia or overgrowth from the periphery remains unclear.

Cystectomy with Peripheral Ostectomy
There are essentially two techniques by which a rim of bone can be removed around a KOT in an attempt to eliminate any remnants of cystic lining and to remove any daughter cysts. In the first technique, en bloc resection is carried out whereby the tumor and a rim of bone are removed in continuity and the tumor itself is not separately removed. In the second technique, the tumor is first enucleated, and a rim of bone approximately 1 mm in thickness is then removed all around the cystic cavity to eliminate any remnants of the lining or daughter cysts. This rim of bone is normally removed with a large pineapple-type burr, and to ensure that bone removal is equal all around, the cavity can be stained with methylene blue or an alternative stain that reaches to a depth of around 1 mm, and then all the stained bone is removed with the burr. Conceptually, it is possible that if there are tumor remnants in this peripheral bone, a pineapple burr could drive them deeper into the bone rather than bringing them out, but this technique nevertheless appears to be successful and lowers the recurrence rate.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


