Introduction
Conventional orthodontic techniques do not intrude posterior teeth effectively, and almost all methods result in anterior extrusion rather than posterior intrusion. New absolute anchorages (miniscrews and miniplates) are said to make posterior tooth intrusion possible. The aim of this study was to evaluate the clinical success of a new method for molar intrusion with miniscrews and its probable accompanying side effects.
Material and methods
Ten women with overerupted upper first molars participated in this study. Upper molar bands with brackets were cemented. Two miniscrews were placed, 1 in the mesiopalatal and another in the mesiobuccal aspect of the upper first molars; a spring made of 0.017 × 0.25-in titanium-molybdenum alloy (TMA) wire was used to apply 100 g of force through the attachments (50 g each side). Molar intrusion and external apical root resorption were evaluated by comparing parallel periapical radiographs with bite blocks at 3 intervals: beginning of treatment (T0), at the end of active treatment (T1), and 6 months after treatment completion (T2).
Results
The mean value of intrusion was 2.1 mm after completion of active treatment. On average, 0.4 ± 0.2 mm relapse had occurred during 6 months of retention, and the mean residual intrusion was 1.7mm, which was statistically significant. Mean root resorption of 0.3 ± 0.2 mm for palatal root and 0.4 mm for mesiobuccal and distobuccal root was measured.
Conclusions
Statistically significant intrusion (2.1 ± 0.9 mm) was obtained during active treatment. The mean value of relapse was 0.4 ± 0.2 mm, and the mean value for residual intrusion was 1.7 ± 0.6 mm. Minor apical root resorption occurred during treatment.
Overextrusion of maxillary molars usually results from early loss of antagonistic teeth. The elongated dentoalveolar process may induce problems such as functional disturbances and occlusal interference and cause great difficulty during prosthetic reconstruction. Conventional options for removing such interference include coronal reduction of molar crown—which often requires root canal therapy—and crown restorations or posterior subapical osteotomy, with the risk of general anesthesia and high cost.
Orthodontic intrusion of molars seemed to be unsuccessful until the development of a skeletal anchorage system. Conventional techniques for intrusion require anchorage reinforcement by incorporating multiple teeth and using extraoral devices that depend heavily on patient cooperation and usually result in extrusion of other teeth rather than posterior intrusion.
Skeletal anchorage, including dental implants, surgical miniplates, and miniscrews, is now growing in popularity because of its ability to provide absolute anchorage. The literature contains several reports of molar intrusion accomplished by miniplates in patients with anterior open bite or overextruded molars. However, compared with miniscrews, miniplates have several disadvantages, including higher cost, limited area for insertion, and the need for 2 separate insertion and removal surgeries.
To date, the available literature for molar intrusion with skeletal anchorage devices, especially miniscrews, consists mainly of case reports and a few animal studies. The literature clearly shows that teeth can be successfully intruded in variable rates ranging from 1.2 mm in Carillo et al’s study to 5 mm in Umemori et al’s study. Intrusion forces also ranged from 50 g in Carillo et al’s study to 500 g in Umemori et al’s study. In some of these studies, elastomeric materials were used for delivering intrusion forces, which may have several shortcomings like rapid force degradation, hygienic problems, and need for patient cooperation. Also, besides elastomeric materials, NiTi coil springs used in some other studies lack the ability to change force vector, which is sometimes needed for controlling molar crown torque during intrusion, and operators were obliged to use lingual or transpalatal arches or brackets on multiple teeth for correcting crown torque.
On the other hand, measuring the amount of intrusion and root resorption in nearly all the human studies was based on lateral cephalog or panoramic images, which are not accurate enough for this application.
The purpose of this study was to introduce a new approach for molar intrusion with miniscrews, with better force consistency and force vector control during treatment, and to evaluate its clinical success and concomitant root resorption by a more accurate method.
Material and methods
Participants
Ten female subjects admitted to the orthodontic department were selected for this study. Their mean age was 43.6 years (25 to 57 years) and each had at least overerupted maxillary first molar, which contributed to prosthodontic replacement of the opposite tooth. None of them had previous orthodontic treatment or active periodontal disease in the beginning of treatment.
Materials
For molar intrusion, we used an Absoanchor Miniscrew Minikit (Dentos Inc, Daegu, Korea), which consists of long and short hand drivers for miniscrew insertion, a round bur (1.9-mm diameter, 21-mm length) for making an indentation in the cortex, and bracket type miniscrews (1.3-mm diameter, 7-mm length).
Stainless steel bands with .018 × .030 welded brackets (Dentaurum, Inspringen, Germany) was banded over extruded teeth. In order to force delivery, a .017 × 0.25-in titanium-molybdenum alloy (TMA) spring was constructed, which was attached to the miniscrew’s head in 1 end and ligated to the bracket in the other end to reach the predetermined force ( Fig I ).

Application of intrusive force
Two miniscrews with bracket-type head were inserted: 1 in the mesiobuccal aspect and another in themesiopalatal aspect of the selected tooth. After a 2-week interval for soft tissue healing, bands with brackets were cemented on the teeth and the .017 × 0.25-in TMA springs were fitted into the slot on the miniscrew’s head and ligated. The other end of the spring was ligated to the bracket that was welded on the band. In order to have just 1 contact point, the spring was not engaged in the bracket slot on the tooth ( Fig I ). By pulling the occlusal arm of the spring with a force gauge hook, it could be adjusted in order to deliver 50 g of force on each side of the tooth. Patients were visited every 4 weeks for spring adjustments and observation of treatment progress.
Radiographic evaluation
We used parallel periapical radiographs with bite blocks to measure the amount of intrusion and root resorption in 3 intervals: at the beginning of treatment (T0), treatment completion (T1), and 6 months after retention (T2). Film-film holder-tube position should have remained the same in these 3 intervals in order to make radiographs comparable. Thus patients’ bite record and film holder position were registered with polyvinylsiloxane material, and at the same time, the horizontal and vertical angles of the tube were recorded for each patient. Radiographs were scanned with a high-resolution scanner (700 dpi) by magnification of 1:1 and were saved in separate files.
In order to have a precise assessment of tooth movement and root resorption, we used a computer software named PLANMECA Dimaxis Classic (PLANMECA USA, Roselle, Ill), which could measure the variables by pixel units and then convert them to millimeters.
Two obvious and distinguishable landmarks in adjacent teeth (like restoration edge or cusp tip) were determined, and a line connecting them was used as the reference axis for further measurements. In order to measure the amount of intrusion in each root, a perpendicular line was drawn from this axis to each root apex. The program automatically calculated the distances in pixel units ( Fig 2 ). The highest intrusion amount between roots was considered the intrusion amount of tooth.
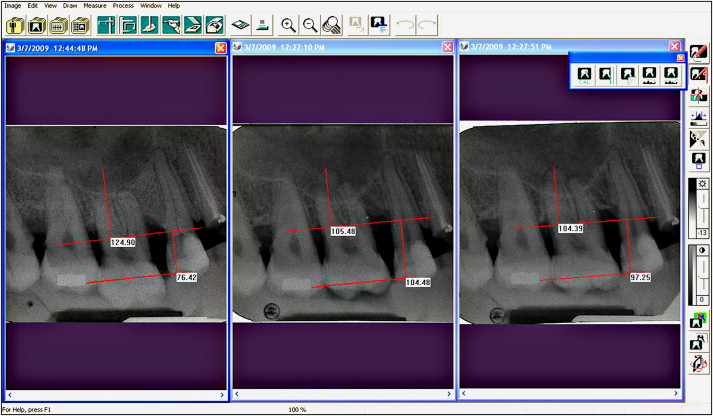
To measure root resorption, a line passing the furcation point of the tooth was drawn parallel to the reference axis, and the perpendicular distance of each root apex to this line was computed in pixel units in 3 time intervals ( Fig 2 ).
A single calibrated examiner was used throughout the study period. In a pilot study on 20 variables, the mean and standard deviation of differences between duplicate measurements of the examiner were 0.02 ± 0.1 mm and considered to be a reflection of intraexaminer reliability.
Finally, by finishing the active treatment (T0-T1), patients were referred for prosthetic replacement of the opposite edentulous area, and during this period they were supposed to use a maxillary acrylic splint as retainer.
Patients were asked for pain and irritation symptoms at each visit during treatment.
Statistical analysis
A 1-sample Kolmogorov-Smirnov test was used for determining normality of the data. Changes in tooth position and root resorption were evaluated by a 1-sample t test, and finally a Spearman correlation test was used to assess the correlations between variables.
Results
The maxillary first molars were successfully intruded in all the patients according to their clinical needs. Mean treatment duration was 7.7 months and ranged from 4.3 to 11.5 months. Changes in tooth position and root resorption during active treatment (T0-T1), retention period (T1-T2), and total treatment (T0-T2) are shown in Table I . The mean intrusion value was 2.1 ± 0.9 mm during active treatment ( P < 0.001), 0.4 ± 0.2 mm relapse took place during the retention period ( P < 0.001). The average amount of intrusion between T0 and T2 was 1.7 ± 0.6 mm ( P < 0.001).
| Variables | Changes during active treatment (T0-T1) | Changes during retention period (T1-T2) | Total change (T0-T2) |
|---|---|---|---|
| Intrusion (mm) | 2.1 ± 0.9 (1.5, 4.5) |
−0.4 ± 0.2 (0.1, –0.7) |
1.7 ± 0.6 (1.1, 2.9) |
| P < 0.001∗ | P < 0.001∗ | P < 0.001∗ | |
| Palatal root resorption (mm) | 0.2 ± 0.2 (0, 0.6) |
0.1 ± 0.2 (0, 0.5) |
0.3 ± 0.2 (0, 0.9) |
| P = 0.08 | P = 0.08 | P = 0.045∗ | |
| Mesiobuccal root resorption (mm) | 0.4 ± 0.3 (0, 0.9) |
0 ± 0.3 (−0.3, 0.4) |
0.4 ± 0.4 (0, 0.9) |
| P = 0.03∗ | P = 0.22 | P = 0.03∗ | |
| Distobuccal root resorption (mm) | 0.2 ± 0.3 (0, 0.8) |
0.2 ± 0.3 (−0.2, 0.6) |
0.4 ± 0.3 (0, 0.8) |
| P = 0.015∗ | P = 0.076 | P < 0.009∗ |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


