We successfully treated a nonsyndromic oligodontia patient with implant-anchored orthodontics and prosthetic restorations. A woman, age 18 years 11 months, had a straight profile and a skeletal Class I jaw-base relationship but had spaced arches because of 7 congenitally missing teeth. After leveling and alignment of the dentition, a titanium miniscrew was temporarily placed at the distal alveolus of the mandibular right first premolar, and the posterior teeth were mesialized to reduce the restorative spaces. After determination of the incisor positions, 3 dental implants were respectively inserted at the sites of the maxillary canines and the mandibular left lateral incisor with guided bone regeneration procedures. Then, screw-retained temporary prostheses were delivered after subepithelial connective tissue grafting and used for molar mesialization as absolute anchorage. After 36 months of active orthodontic treatment, an acceptable occlusion was achieved, both functionally and esthetically, with the 3 dental implants. The maxillary and mandibular molars were mesialized, but the changes of incisor position were minimal. As a result, a proper facial profile was maintained, and an attractive smile was achieved. The resultant occlusion was stable throughout a 3-year retention period. In conclusion, interdisciplinary treatment combined with orthodontics, implant surgery, and prosthodontics was useful for a nonsyndromic oligodontia patient. Especially, the new strategy—implant-anchored orthodontics—can facilitate the treatment more simply with greater predictability.
Oligodontia refers to the congenital absence of many but not all permanent teeth; it is a rare finding. However, orthodontists might encounter this condition because management often requires an integrated orthodontic and restorative approach. The orthodontic treatment of oligodontia is difficult in general because only a few anchorage teeth are available to support tooth movement.
Recently, implant anchorage has been shown to be effective in treating a wide variety of malocclusions. Dental implants, miniplates, and titanium screws have been used as anchorage for orthodontic treatment, and they are often referred to as temporary anchorage devices. Temporary anchorage devices can provide absolute anchorage for tooth movement without the patient’s compliance. The use of miniscrews has gained acceptance among orthodontists and patients because there is little discomfort, they are relatively noninvasive, and there are fewer limitations in placement. Despite their small diameter and short length, miniscrews can provide stable anchorage for various types of tooth movements, including intrusion, retraction, and protraction. Use of temporary anchorage devices is helpful in treating oligodontia patients. As for molar mesialization, we previously reported the successful outcome in an oligodontia patient with titanium screws and extended anchorage wires placed in the retromolar area. However, the mechanics were complicated, and the wires were sometimes difficult to adjust. Thus, a more simple mechanism was needed.
Dental implants are now considered an effective and reliable modality for the rehabilitation of a dentition with missing teeth. However, severely reduced bone quantity caused by the congenital absence of multiple teeth is often found in patients with oligodontia. Therefore, bone augmentation procedures to establish appropriate bone quantity are required in most cases. The surgical procedures should be carefully planned on an individual basis, and their timing is considerably important to facilitate the interdisciplinary treatment. It occasionally makes treatment planning difficult and complicated.
In this case report, we demonstrate the successful outcome of interdisciplinary treatment in a nonsyndromic oligodontia patient. Dental implants were placed with bone augmentation immediately after the leveling and alignment phase, and the implants and a miniscrew were used for absolute anchorage during mesial movement of the posterior teeth.
Diagnosis and etiology
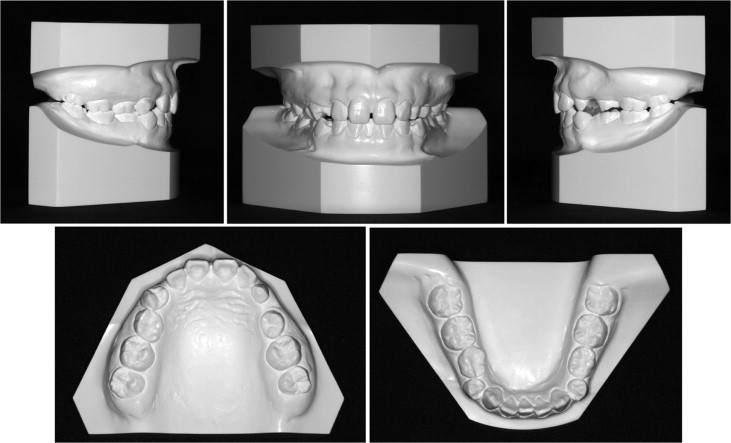
A woman, age 18 years 11 months, had a chief complaint of missing maxillary canines. Her facial profile was straight, and the frontal view was almost symmetrical ( Fig 1 ). The molar relationships were Angle Class I on both sides ( Fig 2 ). Overjet and overbite were both 2.5 mm. Spaced arches were observed in the both dentitions because of the 7 congenitally missing permanent teeth: the maxillary canines, a mandibular incisor, and all second premolars. The maxillary left deciduous canine and all deciduous second molars showed prolonged retention. As for the maxillary first premolars, the right side was rotated distally, and the left was rotated mesially. The maxillary dental midline almost coincided with the facial midline; however, the mandibular dental midline was deviated 3.0 mm to the left.

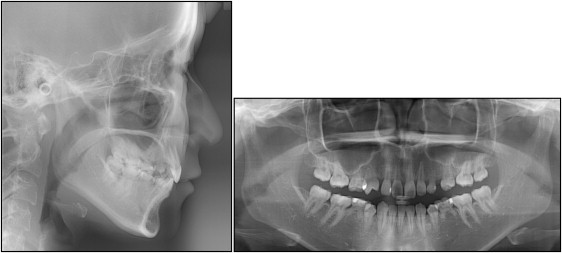
In the panoramic radiograph, root resorption was clearly observed in the maxillary left deciduous canine and the mandibular deciduous molars but was not shown in the maxillary right deciduous molar ( Fig 3 ). The floor of the maxillary sinus was near the roots of the maxillary molars.
The cephalometric analysis, when compared with the Japanese norm, showed a skeletal Class I jaw-base relationship (ANB, 5.0°) ( Table ). The mandibular plane angle was average (MP-FH plane, 27.0°). The maxillary incisors were lingually inclined (U1-FH plane, 102.0°), but the mandibular incisors had an average inclination (L1-MP, 90.0°). As a result, the interincisal angle was significantly increased (IIA, 142.5°).
| Variable | Japanese norm ∗ | SD | Pretreatment | Posttreatment | Postretention |
|---|---|---|---|---|---|
| 18 y 11 mo | 21 y 11 mo | 24 y 11 mo | |||
| Angles (°) | |||||
| ANB | 2.8 | 2.4 | 5.0 | 4.0 | 4.0 |
| SNA | 80.8 | 3.6 | 82.0 | 82.0 | 82.0 |
| SNB | 77.9 | 4.5 | 77.0 | 78.0 | 78.0 |
| Mandiblular plane-Frankfort horizontal plane | 30.5 | 3.6 | 27.0 | 27.0 | 27.0 |
| Gonial angle | 122.1 | 5.3 | 123.0 | 123.0 | 123.0 |
| U1-FH plane | 112.3 | 8.3 | 102.0 | 102.0 | 102.5 |
| L1-Mandibular plane | 93.4 | 6.8 | 90.0 | 90.0 | 90.0 |
| Interincisal angle | 123.6 | 10.6 | 142.5 | 142.5 | 142.0 |
| Occlusal plane | 16.9 | 4.4 | 13.5 | 11.0 | 11.0 |
| Lines (mm) | |||||
| S-N | 67.9 | 3.7 | 69.0 | 69.0 | 69.0 |
| N-Me | 125.8 | 5.0 | 128.5 | 128.5 | 128.5 |
| Me/palatal plane | 68.6 | 3.7 | 70.5 | 71.0 | 71.0 |
| Ar-Go | 47.3 | 3.3 | 47.0 | 47.0 | 47.0 |
| Ar-Me | 106.6 | 5.7 | 112.0 | 113.5 | 113.5 |
| Go-Me | 71.4 | 4.1 | 78.0 | 79.5 | 79.5 |
| Overjet | 3.1 | 1.1 | 2.5 | 2.5 | 2.5 |
| Overbite | 3.3 | 1.9 | 2.5 | 3.0 | 3.0 |
Treatment objectives
The patient was diagnosed as having an Angle Class I malocclusion with a skeletal Class I jaw-base relationship and a spaced arch due to 7 congenitally missing permanent teeth. The treatment objectives were (1) to achieve an acceptable occlusion with a good functional Class I occlusion, (2) to control the available spaces for the dental implants with mesialization of the maxillary and mandibular molars, and (3) to achieve an attractive smile and maintain a proper facial profile. Then, dental implants with bone augmentation were planned for the maxillary canines and the mandibular left lateral incisor.
Treatment objectives
The patient was diagnosed as having an Angle Class I malocclusion with a skeletal Class I jaw-base relationship and a spaced arch due to 7 congenitally missing permanent teeth. The treatment objectives were (1) to achieve an acceptable occlusion with a good functional Class I occlusion, (2) to control the available spaces for the dental implants with mesialization of the maxillary and mandibular molars, and (3) to achieve an attractive smile and maintain a proper facial profile. Then, dental implants with bone augmentation were planned for the maxillary canines and the mandibular left lateral incisor.
Treatment alternatives
Several procedures were explored to achieve an acceptable occlusion. Prosthetic restorations without orthodontic treatment might shorten the total treatment period; however, this required extraction or pulpectomy of some teeth before the restorations. In addition, it is almost impossible to achieve a Class I occlusion and to correct the midline deviation. Therefore, the best plan seemed to be a compromise.
Comprehensive treatment including orthodontics was proposed to improve her specific issues. If the deciduous canine and molars were planned to be maintained as long as possible, the restorations could be minimal in this timing. Meanwhile, the plan could not ensure a stable occlusion over time because the patient was still growing and some root resorption was seen in the deciduous teeth. If the dental implants were placed after extraction of all remaining deciduous molars, an ideal occlusion could be achieved. However, the placement of 7 implants would be expensive and would involve considerable surgical invasion. Therefore, we planned to mesialize both the maxillary and mandibular molars to reduce the spaces for the prosthetic restorations.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


