Introduction
Health-information-seeking behavior is the purposive search for health-related information. The literature contains few articles examining this behavior as it relates to orthodontics; therefore, the aim of this study was to investigate how adolescent orthodontic patients seek information about their treatment, why they search for this information, and how they prefer the information to be available.
Methods
In-depth interviews were conducted with 15 subjects, 10 to 16 years old, who were considering orthodontic treatment. The purpose of the interviews was to identify themes that were then used to develop a questionnaire to investigate information-seeking behavior. The questionnaire was distributed to 50 adolescent orthodontic patients.
Results
The main sources of information were talking to a dentist or an orthodontist (84%), talking to peers (66%), and reading information leaflets (64%). Surprisingly few respondents had used the Internet (8%). The preferred sources of information were talking to an orthodontist (26%) and family members (12%), followed by talking with the general dentist (10%), viewing a DVD (10%), or reading information leaflets (10%).
Conclusions
The preferred method of obtaining information was verbal, followed by audiovisual and written. Audiovisual information could be beneficial for those who find reading difficult or who struggle to retain verbal information. Few patients accessed information via the Internet, and this was attributed to concerns about the reliability of the information.
Health-information-seeking behavior has been defined in the literature as “the purposive search for health-related information to satisfy a query.” Information is an important part of the health care pathway because it is a method of educating patients to allow them to participate in choices about their health and treatment and therefore make informed decisions. Educating patients might encourage their involvement in their own health care decisions and also ensure that they understand the rules, rights, and obligations of health organizations.
Miller and, more recently, Lambert et al highlighted that health-information-seeking behavior can be used as a coping strategy for patients; they divided patients into “monitors” and “blunters.” Those who were monitors actively sought information about their medical condition, and the information helped to reduce anxiety and offer reassurance. Blunters, on the other hand, actively avoided information and preferred less information because they coped by distracting themselves from the situation. Thus, tailoring information to a patient’s coping style is thought to benefit him or her both psychologically and physiologically. Patients who were monitors fared better with more information that helped to reduce anxiety and offer reassurance, whereas the blunters preferred less information because they distracted themselves from threatening situations.
Much of the research carried out in this area involves adult patients and health care interventions for serious and life-threatening medical conditions; there is little research involving children and adolescents or elective procedures. Different age groups have different levels of understanding, and this should be a consideration when planning to provide information. It has been proposed that information provision before a medical procedure can have a positive effect on a child’s anxiety. Claar et al found that improving a child’s knowledge about a forthcoming medical procedure allowed him or her to understand what to expect; therefore, this might reduce the fear of the unknown and also the anxiety level, stress, and pain.
Dental education has been shown to improve children’s knowledge and reduce concerns about treatment, all of which might impact on the patients’ compliance. Habiban et al found that children who were undergoing orthodontic treatment often had little knowledge of their treatment. For a patient to provide a valid consent to treatment, he or she must be able to understand, have time to consider, and be able to ask questions about the nature, purpose, benefits, and risks of the procedures. Patients should also be able to retain the information they are given to prove that they have sufficient understanding of the procedures. Thomson et al investigated retention of information in children and parents after an initial orthodontic consultation. Parents responded better to verbal information than did children, and it was suggested that verbal information given to children should be reinforced with either written or visual information. Patel et al found that patients who received verbal information supplemented by audiovisual information had better retention of it than those who received verbal information supplemented by written information. However, a more recent study found that supplementing verbal information with written information had no effect on patient anxiety in orthodontic clinics.
Different methods of delivering information have been used in health care. Information leaflets are a popular method of supplementing information given by clinicians. However, health literacy can be a barrier to delivery of information; for those with low reading ability, including young patients, it might be time to move away from the traditional information leaflet and use a different method to provide information. The aim of this study was to investigate how adolescent orthodontic patients find information about orthodontic treatment, why they search for this information, and how they prefer the information to be made available.
Material and methods
Ethical approval was granted, and written parental consent and patient assent were obtained. For parts 1 and 2 of the study, patients were included if they were aged between 10 and 16 years, willing to participate in the study, accompanied by a parent or legal guardian who consented to their inclusion, and either had not started treatment or were within 8 weeks of starting fixed appliance treatment. Patients were excluded if they were receiving multidisciplinary treatment, had undergone a previous course of fixed appliance treatment, or were receiving only removable appliance or headgear treatment. A sample size calculation was not appropriate because this study was investigating patients’ opinions, and no hypothesis was being tested. The study was conducted in 2 stages: part 1 used qualitative methods to investigate information-seeking behavior and develop a patient-centered questionnaire, and part 2 involved piloting and distributing the questionnaire.
In part 1, in-depth semistructured interviews were conducted with 15 patients who had not yet begun treatment (6 girls, 9 boys; mean age, 12.9 years) to collect qualitative data and identify themes that could be used to develop a patient-centered questionnaire. Face-to-face interviews were undertaken by 1 researcher (R.S.) in a nonclinical area; the interviewer was a qualified dentist in an orthodontic graduate training program. Interview training was provided by the other researchers (S.J.C. and F.S.R.); both were experienced interviewers who had previously received in-depth interviewer training. The techniques involved were covered over a series of training sessions; 5 practice interviews were then undertaken before the study, and detailed feedback was provided after each interview.
All interviews were recorded and transcribed verbatim into Word format (Microsoft, Redmond, Wash) by the interviewer immediately afterward. A topic guide was used during the interviews, but themes and concepts that arose during the interviews that were relevant to the research question but not in the guide were also fully explored. Interviews were carried out informally with no time pressure, and the interview ended when the patient had no further comments and all relevant topics had been explored. The interviews continued until no new themes arose.
The interviews were analyzed by using content analysis whereby the researcher read the transcripts several times, and sections of the interviews were coded into themes and subthemes. A framework approach, developed by the National Centre for Social Research, was used to manage the data from the interviews. This involved creating a separate workbook in Excel (Microsoft) for each main theme and summarizing the transcripts into the spreadsheet. The columns represented subthemes, and the rows represented each patient; quotes from the interviews were placed in the relevant cells. Using the framework spreadsheet made it easier to visualize interrelationships among the data and to order the subthemes.
The questionnaire was developed, following the principles defined by Williams, from the themes identified in the framework analysis. This process was undertaken by all 3 researchers, 2 of whom were senior clinicians experienced in qualitative research and development of patient-centered questionnaires. The questionnaire was divided into sections that represented the main themes identified in the framework spreadsheet. Most questions had a list of possible responses to choose from, and these were generated from analysis of the interviews. Each participant was allowed to provide additional information after each section, in case his or her views were not included.
The questionnaire was pilot tested on 8 patients to assess its readability and acceptability, and they were asked to make suggestions for improvement. The readability of the questionnaire was assessed by using the Flesch Reading Ease test. Minor changes were made after this: eg, printing the instructions in bold and using duplex printing. The questionnaire is reproduced in the Appendix .
The questionnaire was then distributed in person to 50 patients at the Eastman Dental Hospital’s Orthodontic Department of the University College London Hospitals Foundation Trust in London, United Kingdom, as they attended a routine appointment. The patients either had not started treatment or were within 8 weeks of commencing treatment, as described in the inclusion criteria. They were asked to complete the questionnaire in the department immediately after their appointment, although 1 patient returned the questionnaire by post.
Results
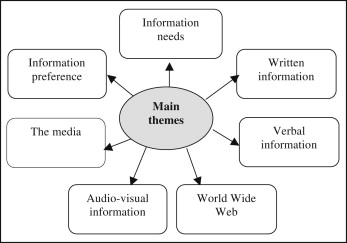
For part 1, questionnaire development, 15 patient interviews were undertaken; the content analysis identified 7 main themes ( Fig 1 ); within each main theme, there were a number of subthemes. The questionnaire was also divided into 7 sections representing the main themes identified, and a section for demographics was also included.
- 1.
Information needs: what patients wanted to know and any anxieties or concerns regarding forthcoming treatment.
- 2.
Written information: if, how, and why patients obtained information in this format.
- 3.
Verbal information: if, how, and why patients obtained information in this format.
- 4.
The World Wide Web: investigated patients’ usual Internet activity, how they use the Internet to search for information, and their concerns regarding the reliability of information on the Internet.
- 5.
Patients’ attitudes toward the media.
- 6.
Patients’ attitudes toward audiovisual information.
- 7.
Preferred source: patients were asked to specify their single preferred method for receiving information about orthodontic treatment.
For part 2, in the pilot study, the questionnaire took an average of 15 minutes to complete (range, 11-18 minutes), and the Flesch Reading Ease score of the questionnaire was 84.8, which corresponds to a reading age of approximately 10 years.
The results of the questionnaire are presented according to the themes from the framework analysis. Fifty-five patients were approached, but 5 patients or their parents refused to participate, giving a response of 91%. Fifty patients completed the questionnaire; 62% were female, and 38% were male. The average age was 12.6 years (SD, 1.5 years).
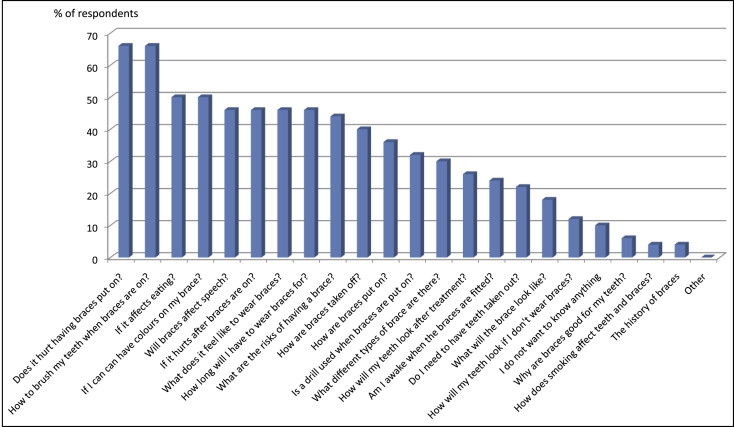
The second section enquired how patients found information about orthodontics and what they wanted to know about wearing an appliance. Most patients (84%) said that they had found information about their future treatment by talking to the family dentist or an orthodontist. Over half of patients also obtained information by talking to friends (66%) and parents (60%), and from reading an information leaflet (64%). Fewer patients had talked to other family members (28%), siblings (20%), watched television (10%), or looked on the Internet (8%) for information. Most patients wanted to know whether having a brace fitted hurts (66%), how to brush their teeth once a brace had been fitted (66%), and whether it would affect their eating (50%) or speech (46%). Some patients wanted to know exactly how a brace was fitted (36%), whether a drill would be used (32%), and whether they would be awake during this procedure (24%). Forty percent of the patients also wanted to know how a brace would be taken off ( Fig 2 ).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


