Introduction
The etiology of palatal canine impaction is multifactorial and includes a genetic contribution. The aim of this study was to find the incidence and effects of genetic factors on palatally impacted canines in a genetically isolated community of ultraorthodox Hassidic Jews of Ashkenazi decent.
Methods
For this study, we retrospectively evaluated 1000 charts of Hassidic Jewish patients. Their distribution was 58% female and 42% male, with a mean age of 14 years.
Results
From those patients, 49 (4.9%) were determined to have canine impaction. Of these 49, 69.4% had unilateral palatal impaction, 26.5% had bilateral palatal impaction, and 4.1% had unilateral labial impaction. The z-test of proportion showed that female patients have a greater percentage than males for unilateral palatal impaction ( P <0.01) with left-side dominance ( P <0.01).
Conclusions
Our results imply that genetics plays a significant role in maxillary canine palatal impaction. A genetically isolated Hassidic Jewish community can be a useful group to study the effects of genetic factors on various dental anomalies, including palatally displaced canines.
Maxillary canine impaction is a multifactorial dental anomaly commonly encountered in orthodontic practice, with an incidence in the range of 0.8% to 2.8%. After the third molar, it is the most commonly impacted tooth. Palatal impaction is reported to be more prevalent than labial impaction, and unilateral is more common than bilateral. Female patients also have a higher incidence of canine impaction. The etiology is multifold and can be related to the following factors: long tortuous path of eruption, tooth size and arch length discrepancies, arch width deficiencies, microform or absent lateral incisors, familial tendency, genetics, population differences, lack of resorption of the deciduous canine root, abnormal position of the tooth bud, presence of an alveolar cleft, and cystic or neoplastic formation.
Currently, 2 opposing theories—the genetic origin and the guidance theories—are popular for the etiology of a palatally displaced canine (PDC). The proponents of the genetic origin support their theory based on the following 5 evidential categories: occurrence of other dental anomalies concomitant with PDC, bilateral occurrence of PDC, sex differences in PDC occurrence, familial occurrence of PDC, and population differences in PDC occurrence. However, guidance theorists argue that the associated genetic dental anomalies, such as small, missing, and peg-shaped lateral incisors, create an environmentally generated alteration in the eruption pattern of the canine. Furthermore, because many dental anomalies also occur bilaterally more often in female patients, and strong evidence is lacking to disapprove the guidance theory, they still question the validity of genetic origin as the etiology.
The aim of this study was to determine the incidence of impacted canines in a genetically isolated Jewish community to further elucidate the role of genetics in PDC. A better understanding of genetics by clinicians might ultimately lead to better treatment because genetics accounts for variable responses to treatment among different people. The subjects of this study—Hassidic Jews in an ultraorthodox community of Ashkenazi decent—are of specific interest because they live in a society with a mostly homogeneous ethnic background. The resultant inbreeding manifests itself in a host of behavioral and genetically dependent parameters, in which scant normal occlusion can be included.
Material and methods
The charts of 1000 Hassidic Jewish patients were evaluated retrospectively from a private practice in Borough Park of Brooklyn, New York, catering to the Hassidic Jewish subpopulation. The charts were selected randomly, and the distribution of the patients was 58% female and 42% male, with a mean age of 14 years. A canine was considered impacted if it was not erupted within the normal chronologic age range and had to be surgically exposed to bring it into the oral cavity. Incidence, age, sex, location, tooth size and arch length deficiencies, arch width deficiency, sector analysis, angulations, and bilateral occurrence were evaluated.
Location was determined by clinical notes and affirmed by models, photographs, and radiographs.
Tooth size and arch length deficiencies were determined by measurements from models with a sharpened caliper with an accuracy of 0.01 mm (Beerendonk Caliper, Pearson Dental, Sylmar, Calif). Arch length was measured from the mesial aspect of the maxillary first molar to the mesial aspect of the contralateral maxillary first molar. Tooth size was measured from the second premolar to the contralateral second premolar. Tooth size and arch length deficiencies were recorded in millimeters.
Arch width deficiency was determined for both intermolar and interfirst premolar locations. Intermolar width was measured on models from the mesial lingual cusp of the maxillary first molar to the mesial lingual cusp of the contralateral maxillary first molar, and from the central fossa of the mandibular first molar to the central fossa of the contralateral mandibular first molar. Any deficiency in maxillary intermolar arch width was recorded in millimeters. Interfirst premolar width was also measured on the models from the lingual cusp of the maxillary first premolar to the lingual cusp of the contralateral maxillary first premolar, and from the distal lingual fossa of the mandibular first premolar to the distal lingual fossa of the contralateral mandibular first premolar. The discrepancies between maxillary and mandibular measurements were noted in millimeters.
Sector analysis was determined by the canine relationship to the adjacent lateral incisor from the panoramic radiograph.
Sector I: canine is located distally to the distal margin of the lateral incisor.
Sector II: canine is located between the distal margin and the midaxial plane of the lateral incisor.
Sector III: canine is located between the midaxial plane and the mesial margin of the lateral incisor.
Sector IV: canine is located mesially to the mesial margin of the lateral incisor.
Angulation was measured, by using a panoramic radiograph, from the midline between the central incisors to the midaxial plane of the impacted canine.
Statistical analysis
The significance of the difference in the numbers of patients with canine impactions in male vs female patients was evaluated by using the z-test for proportions. The significance of differences in the percentages of patients with right or left dominance of the impaction between the sexes was evaluated by using the z-test for proportions.
Values of arch length, width, and angulation were expressed as mean plus or minus the standard error of the mean (SEM). The significance of differences in arch length, width, or angulation values between the unilateral, bilateral, and labial groups was separately evaluated by using 1-way analysis of variance (ANOVA).
Results
From 1000 patients, 49 (4.9%) were determined to have canine impactions that required surgical exposure and orthodontic traction to facilitate eruption into the arch. Of these, 34 (69.4%) had unilateral palatal impaction, 2 (4.1%) had unilateral labial impaction, and 13 (26.5%) had bilateral palatal impaction.
The location was evaluated by sex in relation to right, left, and bilateral distribution for palatally impacted canines ( Table ). In the unilateral group, female subjects represented a greater percentage (24 of 34, or 70.5%) than males, with right-side distribution of 6 (33.3%) and left-side distribution of 18 (66.7%). Male subjects had 10 of 34 (29.5%) unilateral palatally impacted canines, with right-side distribution of 4 (40%) and left-side distribution of 6 (60%). The bilateral group of 13 patients had 7 females (53.8%) and 6 males (46.2%). The z-test for proportion showed that females represented a greater percentage of total impactions than did males ( P <0.01). Among the unilateral palatal impactions, females showed a statistically significant left-side dominance ( P <0.01).
| Unilateral palatal right |
Unilateral palatal left |
Bilateral palatal |
Labial | Total (n) | % | |
|---|---|---|---|---|---|---|
| Female | 6 | 18 | 7 | 1 | 32 | 65.3 |
| Male | 4 | 6 | 6 | 1 | 17 | 34.7 |
| Total (n) | 10 | 24 | 13 | 2 | 49 | |
| % | 20.4 | 49.0 | 26.5 | 4.1 | 100 |
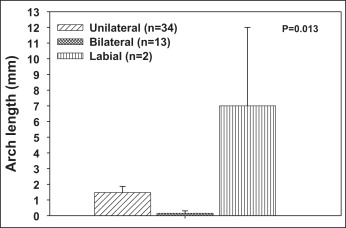
Tooth size and arch length deficiencies ( Fig 1 ) were evaluated for the unilateral palatal, bilateral palatal, and labial impactions. Of the unilateral palatally impacted canines, 22 of 34 (64.7%) showed no arch length deficiency, with a total mean of 1.47 mm of arch length deficiency. The labially impacted canines showed a mean arch length deficiency of 7 mm. The bilateral group showed 12 of 13 (92.3%) with no arch length deficiency and a mean of 0.15 mm.
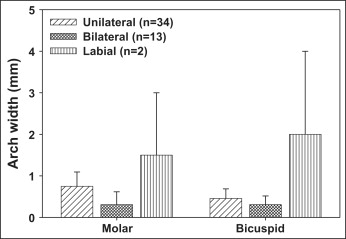
Arch width deficiency ( Fig 2 ) was evaluated for intermolar and interfirst premolar in relation to unilateral palatal, bilateral palatal, and labial impactions. The unilateral palatal group showed 29 of 34 (85.3%) with no intermolar arch width deficiency and a mean intermolar arch width deficiency of 0.75 mm. Similarly, 30 of 34 (88.2%) had no interfirst premolar deficiency, with a mean interfirst premolar deficiency of 0.45 mm. The labial group showed a mean intermolar arch width deficiency of 1.5 mm and a mean interfirst premolar deficiency of 2 mm. The bilateral group had 12 of 13 (92.3%) with no intermolar width deficiency and a mean intermolar arch width deficiency of 0.30 mm. Similarly, 12 of 13 (92%) had no interfirst premolar deficiency and a mean interfirst premolar deficiency of 0.15 mm.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


