Fixed retainers are effective in maintaining the alignment of the anterior teeth more than 90% of the time, but they can produce inadvertent tooth movement that in the most severe instances requires orthodontic retreatment managed with a periodontist. This is different from relapse into crowding when a fixed retainer is lost. These problems arise when the retainer breaks but remains bonded to some or all teeth, or when an intact retainer is distorted by function or was not passive when bonded. In both instances, torque of the affected teeth is the predominant outcome. A fixed retainer made with dead soft wire is the least likely to create torque problems but is the most likely to break. Highly flexible twist wires bonded to all the teeth appear to be the most likely to produce inadvertent tooth movement, but this also can occur with stiffer wires bonded only to the canines. Orthodontists, general dentists, and patients should be aware of possible problems with fixed retainers, especially those with all teeth bonded, because the patient might not notice partial debonding. Regular observations of patients wearing fixed retainers by orthodontists in the short term and family dentists in the long term are needed.
Highlights
- •
Passive and securely bonded fixed anterior retainers are an effective way to prevent posttreatment relapse but require regular supervision.
- •
Small-diameter flexible spiral wires bonded to each tooth pose the greatest risk for creating significant inadvertent tooth movement and resulting complications.
- •
Early detection of bonding failures, wire breakage, and tooth movement created by the retainer is critical in preventing major problems.
- •
A patient with a fixed retainer should be seen regularly by the general dentist if not by the orthodontist, and the orthodontist should accept responsibility for dealing with problems if they arise.
- •
Interaction with a periodontist using bone induction procedures is needed for retreatment of patients with severely displaced teeth.
The stability of orthodontic treatment is a major concern to both orthodontists and patients. Several long-term studies have demonstrated a strong tendency for relapse of anterior alignment after orthodontic treatment and retention. For this reason, many orthodontists believe that permanent retention with a fixed retainer is the only way to maintain ideal dental alignment after treatment. Examining patients on 20-year recall, Booth et al found that periodontal health was better in those whose mandibular fixed retainers bonded only to the canines were still in place than in those whose retainers had been lost or removed, so it appears that permanent retainers are not a risk factor for periodontal problems.
It has been shown that a higher percentage of patients with fixed retainers secured only to the canines will have incisor irregularity at 5 years after treatment than if the retainer wire is bonded to the incisors as well. This has led to increased use of bonding to all teeth, but problems can arise when this is done. Bonding 6 teeth rather than 2 increases the chance of a bond failure within the first 5 years from approximately 20% to 30%. A more serious problem is major inadvertent tooth movement created by a lingual retainer, which has been the subject of previous case reports but has been considered highly unusual.
Tooth movement produced by a fixed retainer is different from the mild relapse seen occasionally despite the presence of a retainer, especially since it is almost never in the direction of the pretreatment position of the tooth and therefore is not relapse. This article was inspired by a patient who was referred to the office of the senior author (T.G.S.) in 2013 with surprising and unexpected mandibular anterior tooth movement and periodontal damage despite an intact small-diameter fixed retainer wire bonded to each tooth. Her coordinated periodontic-orthodontic treatment is discussed below. Through word of mouth among a few colleagues, a dozen or so other examples of tooth movement created by a fixed lingual retainer were collected, providing an impression of the unrecognized extent of the problem.
Our objectives in this article were to illustrate examples of inadvertent tooth movement created by fixed lingual retainers, discuss the most likely causes, make recommendations for prevention and retention management, and discuss the periodontist-orthodontist interactions in retreatment to correct severe problems.
Examples of retainer-created inadvertent tooth movement
No single fixed retainer type appears to be immune to unexpected and unwanted tooth movement, although tooth movement is more likely when more flexible wires are used.
However, different types of tooth movement and problems are specific to the various retainer designs and wire sizes. This is discussed below relative to the most common fixed retainer types: (1) canine-to-canine plain steel wire (0.025-0.032 in) retained with bonding only to the canines, (2) more flexible 0.032-in spiral wire bonded only to the canines, (3) smaller diameter (0.0195-0.0215 in) and increasingly flexible spiral wire bonded to each anterior tooth, and (4) dead soft wire of various dimensions bonded to each anterior tooth.
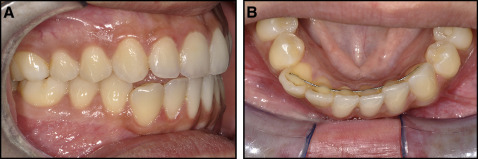
Loss of alignment from inadvertent tooth movement is more likely when wires break. This appears to be most likely with smaller diameter dead soft wires ( Fig 1 ), but it also occurs with small flexible spiral wires bonded to each tooth. Breakage can lead to no retention at all when a wire segment is missing or can lead to independent tooth movement produced by a remaining wire segment ( Fig 2 ).


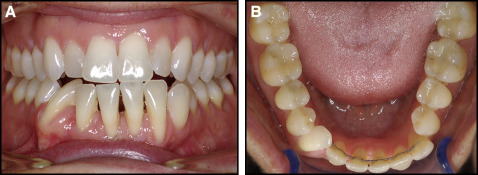
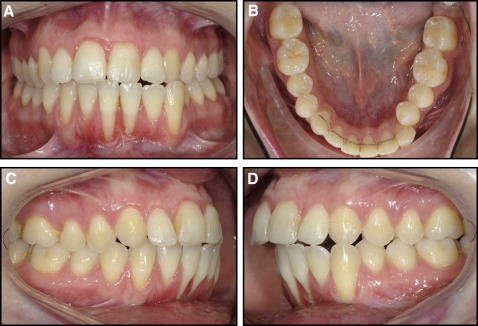
Transverse changes in the position of one or both canines can occur with small wires bonded to each tooth and are seen with both dead soft wires ( Fig 3 ) and flexible spiral wires ( Fig 4 ). Different types of transverse changes occur with larger diameter wires. A stiffer wire produces a more dependent relationship between the canines than does a smaller wire. Twisting of the wire can result in reciprocal movement of the canines and skewing of the arch form ( Fig 5 ). Downward deflection of a relatively stiff wire can produce expansion across the canines ( Fig 6 ).
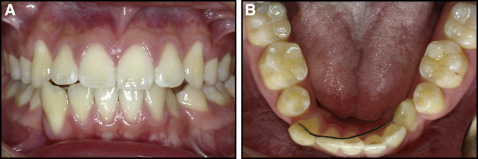
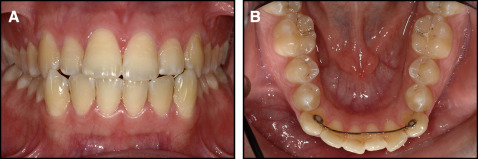
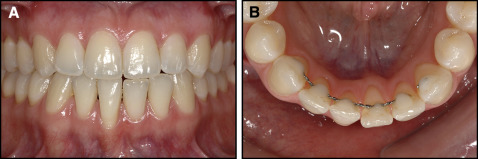
Torque discrepancies between adjacent incisors are most likely with smaller diameter flexible spiral wires ( Fig 7 ), but these can also occur with dead soft wires ( Fig 8 ). In some cases, tooth movement is severe enough to cause periodontal damage ( Fig 9 ). We observed no examples of torque discrepancies between adjacent incisors with larger diameter canine-to-canine wires secured to the canines only.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


