Introduction
The aims of this study were to systematically review the available literature regarding in-vitro orthodontic shear bond strength testing and to analyze the influence of test conditions on bond strength.
Methods
Our data sources were Embase and Medline. Relevant studies were selected based on predefined criteria. Study test conditions that might influence in-vitro bond strength were independently assessed by 2 observers. Studies reporting a minimum number of test conditions were included for meta-analysis by using a multilevel model with 3 levels, with author as the highest level, study as the second level, and specimens in the study as the lowest level. The primary outcome measure was bond strength.
Results
We identified 121 relevant studies, of which 24 were included in the meta-analysis. Methodologic drawbacks of the excluded studies were generally related to inadequate reporting of test conditions and specimen storage. The meta-analysis demonstrated that 3 experimental conditions significantly affect in-vitro bond strength testing. Although water storage decreased bond strength on average by 10.7 MPa, each second of photopolymerization time and each millimeter per minute of greater crosshead speed increased bond strength by 0.077 and 1.3 MPa, respectively.
Conclusions
Many studies on in-vitro orthodontic bond strength fail to report test conditions that could significantly affect their outcomes.
Orthodontic bonding of brackets to teeth is a standard procedure to align teeth with fixed appliances. Orthodontic treatment with brackets generally takes approximately 2 years. Bond failure of brackets during this period retards treatment and is costly in terms of time, material, and patient inconvenience. Bracket debonding at the end of the treatment should not damage the enamel. Hypothetically, in-vivo testing in controlled trials is the best way to test the effectiveness of a bonding system and any detrimental effects on the enamel. However, clinically, it is almost impossible to distinguish the adhesive potential of a specific bonding system independent of many other variables that can influence either the quality or the longevity of bracket bonding to enamel. In addition, the methodologic quality of in-vivo randomized controlled trials (RCTs) evaluating debonding and bracket failure is generally poor. Consequently, it is difficult to draw conclusions about the effectiveness of specific bonding systems and their effects on the enamel from in-vivo studies.
In-vitro studies possibly allow for more standardized procedures for testing a specific bonding system. However, the various test conditions that are used hamper the comparison of their results. Test conditions suggested to influence bond strength include enamel origin (ie, bovine vs human), substrate storage (eg, physiologic saline solution or water), and pretreatment of the enamel surface (eg, grinding and means of cleaning). In addition, bond strength testing might also be influenced by the specific test mode used (eg, tensile or shear testing). An explanation for the different outcomes between in-vitro bond strength studies might therefore be that bond strength is not being tested but, rather, an unknown combination of mechanical properties and factors related to the test surfaces. Lately, more attention has been given to the various test conditions and their effects on the results. Recent studies have evaluated the influence of some of these factors on bond strength, including force location, tooth type, crosshead speed variations, and loading mode.
At present, there is no overview on bracket bond strength from which general conclusions can be drawn. Because of the lack of standardization, the growing number of in-vitro studies being published can only be evaluated individually. The aims of this study were to systematically review the literature regarding in-vitro bond strength and failure mode of the most frequently used clinical bonding systems and to analyze by meta-regression the influence of test conditions on the bond strength measured.
Material and methods
Relevant studies were identified in a literature search and subsequently selected on the basis of inclusion criteria. Studies fulfilling the inclusion criteria were assessed for reporting test conditions that could influence the results of in-vitro bond strength testing. The studies reporting a minimal number of test conditions were included for meta-analysis.
To identify studies related to in-vitro bond strength, a search was performed in the databases of Medline (1967 to December 2007) and Embase (1950 to December 2007) ( Table I ). References of identified studies and relevant review articles were searched for additional studies missed in the initial search. English was the language restriction.
| Search | Literature search strategy |
|---|---|
| 1 | Explode “orthodontic-brackets”/MeSH all subheadings |
| 2 | Bracket∗ |
| 3 | Fixed applian∗ |
| 4 | #1 or #2 or #3 |
| 5 | Explode “dental-bonding”/MeSH all subheadings |
| 6 | Bond∗ |
| 7 | #5 or #6 |
| 8 | #4 and #7 |
| 9 | Explode “composite-resins”/MeSH all subheadings |
| 10 | Explode “compomers”/MeSH all subheadings |
| 11 | Explode “glass-ionomer-cements”/MeSH all subheadings |
| 12 | Composite resin |
| 13 | Glass ionomer |
| 14 | Compomer |
| 15 | #8 and (#9 or #12) |
| 16 | #8 and (#10 or #14) |
| 17 | #8 and (#11 or #13) |
| 18 | #8 and bond strength |
| 19 | Search Medline/Embase: #15 or #16 or #17 or #18 |
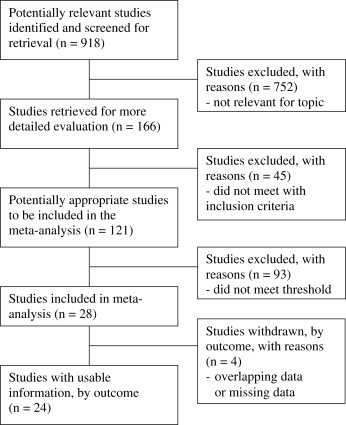
Initially, the titles and abstracts of the studies identified in the literature search were prescreened (by K.J.F.) for relevance to the topic of this study (in-vitro orthodontic shear bond strength testing). The full text of each possibly relevant study was retrieved and assessed by 2 reviewers (M.Ö., K.J.F.) for inclusion and detailed assessment of the experimental conditions. The Figure outlines the algorithm of the study selection procedure.
Studies regarding bond strength testing were selected for detailed assessment of the experimental conditions if they met the following criteria: in-vitro investigation, with the shear bond strengths of metal brackets evaluated and expressed in megapascals (MPa), and the sound buccal enamel of human premolars used. Case reports, abstracts, letters, and narrative reviews were excluded.
A list of 27 items was used to assess the experimental conditions, each reflecting an experimental condition that influences the results of in-vitro bond strength testing ( Table II ). Before the assessment of the studies, 2 observers (M.Ö. and K.J.F.) discussed all 27 experimental conditions to reach consensus about their content. They independently assessed whether the experimental conditions were reported in the study. After the assessment, the observers agreed on the reporting of the 27 experimental conditions of each study in a consensus meeting.
| Experimental condition | Number (%) of studies adequately reporting experimental condition |
|---|---|
| 1. Substrate origin ∗ | 121 (100) |
| 2. Type of teeth ∗ | 121 (100) |
| 3. Storage time before bonding | 38 (31) |
| 4. Storage temperature before bonding | 38 (31) |
| 5. Storage solution before bonding † | 108 (89) |
| 6. Cleaning of specimens † | 113 (93) |
| 7. Bracket material ∗ | 121 (100) |
| 8. Type of bracket † | 94 (78) |
| 9. Type of etchant † | 111 (92) |
| 10. Time of etching † | 109 (90) |
| 11. Adhesive type † | 119 (98) |
| 12. Amount of force at bracket placement | 18 (15) |
| 13. Light device type † | 75 (62) |
| 14. Total polymerization time † | 84 (69) |
| 15. Light directions | 65 (54) |
| 16. Sample storage time † | 109 (90) |
| 17. Sample storage solution | 103 (85) |
| 18. Sample storage temperature | 97 (80) |
| 19. Thermocycling | 26 (22) |
| 20. Testing machine | 119 (98) |
| 21. Shear testing as test method | 121 (100) |
| 22. Crosshead speed † | 117 (97) |
| 23. Force location on bracket † | 83 (69) |
| 24. Blade design † | 73 (60) |
| 25. ARI | 93 (77) |
| 26. Magnification used in determining ARI | 70 (58) |
| 27. Bond strength in MPa ∗ | 121 (100) |
∗ Studies reporting experimental conditions numbers 1, 2, 7 and 27 were included in the systematic review.
† Studies reporting experimental conditions numbers 5, 6, 8, 9, 10, 11, 13, 14, 16, 22, 23 and 24, together with those conditions marked ∗, were selected for meta-analysis.
Studies included in the meta-analysis
The 2 observers independently determined the most relevant experimental conditions for in-vitro bond strength studies based on the results from previous studies. In a consensus meeting, agreement was reached on these required experimental conditions. Studies were included in the meta-analysis if at least all of the following experimental conditions were reported: storage solution of teeth, cleaning of enamel, bracket type, etchant type, etching time, adhesive type, photopolymerization device, total photopolymerization time, specimen storage time, crosshead speed, force location on bracket, and blade design of the jig of the universal testing machine.
The 2 observers independently extracted the data. Consensus was reached after discussion in case of disagreement.
First, for each of the 27 experimental conditions, the number and percentage of included studies describing this specific item were calculated ( Table II ). Subsequently, for each study included in the meta-analysis, the following data were presented: thymol storage solution (yes/no), fluor-free cleaning (yes/no), mesh brackets (yes/no), phosphoric acid etching (yes/no), etching time (<30 seconds/≥30 seconds), photopolymerization time (seconds), photopolymerized composite (yes/no), halogen light (yes/no), water storage (yes/no), storage time (hours), thermocycling (yes/no), crosshead speed (millimeters per minute), force location on the tooth-bracket interface (yes/no), and shearing blade (yes/no). Of the latter data, the influence on the main outcome variable (bond strength in megapascals) was evaluated in the meta-analysis. Failure mode reported with the adhesive remnant index (ARI) was also scored when reported and is presented as the percentage of specimens with all adhesive left on the enamel.
Statistical analysis
Statistical analyses were performed by using the Statistical Package for the Social Sciences (version 16.0, SPSS, Chicago, Ill). The interobserver agreement with respect to the reporting of experimental conditions of the included studies before the consensus meeting was expressed as the Cohen kappa. For descriptive statistics, means (standard deviations or medians) and interquartile ranges in skewed distributions are reported. In MLwin (version 2.02, Centre for Multilevel Modelling, Bristol, United Kingdom), a 3-level analysis (random-effects model) was performed. This is a meta-regression analysis. The lowest level corresponded to the specimen level (specimens in studies), the middle level with the study, and the highest level corresponded with the author. In this way, the correlation within authors between studies was taken into account. Residual variance was entered in the multilevel model by using the within-study variance published in each study.
Different models were compared by using the change in deviance (–2 log likelihood), a likelihood ratio test (chi-square distributed). In this way, it was also possible to test the statistical heterogeneity between authors and between articles by making different assumptions about (models for) the covariance structure. Effects with P values smaller than 0.05 were considered significant.
Results
The searches of Medline and Embase yielded 918 publications. After the first assessment, 166 studies were judged to be relevant for this systematic review. We found no additional studies by checking the references of the included studies and relevant review articles. After we used the specified criteria, 121 of the 166 studies regarding bond strength testing were included for detailed assessment of the experimental conditions ( Fig ). Interobserver agreement (Cohen kappa) for reporting the 27 experimental conditions of the included studies was 0.86. Disagreements were generally caused by differences in language interpretation and were resolved in the consensus meeting.
On average, the 121 included studies reported a mean of 20.4 (SD, 2.8) experimental conditions with a minimum of 12 and a maximum of 26. The most poorly reported item was the experimental condition of amount of force at bracket placement. This was reported in 18 (15%) of the 121 studies. The most relevant experimental conditions for in-vitro bond strength were reported in the following percentage of studies: adhesive type, 98%; crosshead speed, 97%; cleaning of enamel, 93%; etchant type, 92%; etching time, 90%; specimen storage time, 90%; storage solution of teeth before bonding, 89%; bracket type, 78%; total polymerization time, 69%; force location on bracket, 69%; photopolymerization device, 62%; and blade design, 60% ( Table II ).
Studies included for meta-analysis
By using the threshold value, 28 studies were included in the meta-analysis. In 3 of the 9 studies from the same authors, overlapping study data were reported. These duplicated data were not entered in the meta-analysis. One other study was excluded from the meta-analysis because the standard deviation of the main outcome measure (bond strength in megapascals) was not reported. As a result, 24 studies were included in the meta-analysis ( Appendix ). From these studies, data regarding experimental groups with a photopolymerized adhesive and nonself-ligating metal brackets were extracted for further analyses. This yielded 65 experimental groups that tested bond strength in specimen groups ranging from 5 to 40 premolars (mean, 14.1; SD, 7.4) ( Appendix ). Extracted teeth were stored in distilled water with thymol in 30 experimental groups. Fluor-free cleaning was explicitly reported in 32 groups. In 58 groups, a metal bracket with a mesh base was used. Phosphoric acid etching was used in 47 groups; in 48 experimental groups, the etching time was ≥30 seconds. The total polymerization times in the 65 groups varied from 2 to 60 seconds (mean, 25.3; SD, 14.8).
A photopolymerized composite was used in 59 groups, and a halogen polymerization device was used to cure the adhesives in 48 groups. Water storage was reported in 57 groups; in 8 experimental groups, artificial saliva was used for storing the test specimens. The storage times of the specimens ranged from 0 to 672 hours (median, 24; interquartile range, 0-48). Thermocycling was explicitly reported in 15 of the 65 groups. The crosshead speeds when removing the bracket varied from 0.1 to 5.0 mm per minute (median, 0.5; interquartile range, 0.5-1.0). In 23 studies, the force location was at the bracket-enamel interface. In 50 groups, a shearing blade was used for debonding the brackets. In the remaining 15 groups, a wire loop was used for the same purpose. Based on the diversity in reported test conditions, we concluded that there was considerable clinical heterogeneity in these studies. Bond strengths ranged from 3.5 to 27.8 MPa (mean, 13.4; SD, 5.7). ARI scores were reported in 57 experimental groups. Specimens with all adhesive left on the enamel after bond strength testing varied from 0% to 90%.
Meta-analysis
Table III summarizes the results of the meta-analysis. Heterogeneity between authors and studies was still significant after entering the predictor variables ( P <0.05). The results of bond strength testing were negatively influenced when the teeth were stored in water. Water storage on average decreased bond strength by 10.7 MPa, assuming that the other predictors remain constant. Analogously, each second of photopolymerization time increased the bond strength by 0.077 MPa; when crosshead speed increased by 1 mm per minute, bond strength increased by 1.3 MPa.
| Independent variable | Beta (SE) | Lower 95% CI | Upper 95% CI |
|---|---|---|---|
| Water storage (no, 0; yes,1) | –10.648 (3.541) | –17.730 | –3.566 |
| Polymerization time (per second) | 0.077 (0.030) | 0.017 | 0.137 |
| Crosshead speed (mm/min) | 1.302 (0.599) | 0.104 | 2.500 |
| Constant | 20.014 (3.452) | 13.110 | 26.918 |
Results
The searches of Medline and Embase yielded 918 publications. After the first assessment, 166 studies were judged to be relevant for this systematic review. We found no additional studies by checking the references of the included studies and relevant review articles. After we used the specified criteria, 121 of the 166 studies regarding bond strength testing were included for detailed assessment of the experimental conditions ( Fig ). Interobserver agreement (Cohen kappa) for reporting the 27 experimental conditions of the included studies was 0.86. Disagreements were generally caused by differences in language interpretation and were resolved in the consensus meeting.
On average, the 121 included studies reported a mean of 20.4 (SD, 2.8) experimental conditions with a minimum of 12 and a maximum of 26. The most poorly reported item was the experimental condition of amount of force at bracket placement. This was reported in 18 (15%) of the 121 studies. The most relevant experimental conditions for in-vitro bond strength were reported in the following percentage of studies: adhesive type, 98%; crosshead speed, 97%; cleaning of enamel, 93%; etchant type, 92%; etching time, 90%; specimen storage time, 90%; storage solution of teeth before bonding, 89%; bracket type, 78%; total polymerization time, 69%; force location on bracket, 69%; photopolymerization device, 62%; and blade design, 60% ( Table II ).
Studies included for meta-analysis
By using the threshold value, 28 studies were included in the meta-analysis. In 3 of the 9 studies from the same authors, overlapping study data were reported. These duplicated data were not entered in the meta-analysis. One other study was excluded from the meta-analysis because the standard deviation of the main outcome measure (bond strength in megapascals) was not reported. As a result, 24 studies were included in the meta-analysis ( Appendix ). From these studies, data regarding experimental groups with a photopolymerized adhesive and nonself-ligating metal brackets were extracted for further analyses. This yielded 65 experimental groups that tested bond strength in specimen groups ranging from 5 to 40 premolars (mean, 14.1; SD, 7.4) ( Appendix ). Extracted teeth were stored in distilled water with thymol in 30 experimental groups. Fluor-free cleaning was explicitly reported in 32 groups. In 58 groups, a metal bracket with a mesh base was used. Phosphoric acid etching was used in 47 groups; in 48 experimental groups, the etching time was ≥30 seconds. The total polymerization times in the 65 groups varied from 2 to 60 seconds (mean, 25.3; SD, 14.8).
A photopolymerized composite was used in 59 groups, and a halogen polymerization device was used to cure the adhesives in 48 groups. Water storage was reported in 57 groups; in 8 experimental groups, artificial saliva was used for storing the test specimens. The storage times of the specimens ranged from 0 to 672 hours (median, 24; interquartile range, 0-48). Thermocycling was explicitly reported in 15 of the 65 groups. The crosshead speeds when removing the bracket varied from 0.1 to 5.0 mm per minute (median, 0.5; interquartile range, 0.5-1.0). In 23 studies, the force location was at the bracket-enamel interface. In 50 groups, a shearing blade was used for debonding the brackets. In the remaining 15 groups, a wire loop was used for the same purpose. Based on the diversity in reported test conditions, we concluded that there was considerable clinical heterogeneity in these studies. Bond strengths ranged from 3.5 to 27.8 MPa (mean, 13.4; SD, 5.7). ARI scores were reported in 57 experimental groups. Specimens with all adhesive left on the enamel after bond strength testing varied from 0% to 90%.
Meta-analysis
Table III summarizes the results of the meta-analysis. Heterogeneity between authors and studies was still significant after entering the predictor variables ( P <0.05). The results of bond strength testing were negatively influenced when the teeth were stored in water. Water storage on average decreased bond strength by 10.7 MPa, assuming that the other predictors remain constant. Analogously, each second of photopolymerization time increased the bond strength by 0.077 MPa; when crosshead speed increased by 1 mm per minute, bond strength increased by 1.3 MPa.
| Independent variable | Beta (SE) | Lower 95% CI | Upper 95% CI |
|---|---|---|---|
| Water storage (no, 0; yes,1) | –10.648 (3.541) | –17.730 | –3.566 |
| Polymerization time (per second) | 0.077 (0.030) | 0.017 | 0.137 |
| Crosshead speed (mm/min) | 1.302 (0.599) | 0.104 | 2.500 |
| Constant | 20.014 (3.452) | 13.110 | 26.918 |
Discussion
There was great diversity in the experimental conditions of studies reporting bond strength testing in orthodontics. The results from the meta-analysis in this systematic review indicate that the experimental conditions of water storage, photopolymerization time, and crosshead speed significantly influenced the results of in-vitro bond strength testing.
As previously shown in 2 other reviews evaluating orthodontic bond strength studies, there is still great diversity in test protocols and quality of these studies. The observed heterogeneity between the studies in this meta-analysis was clinically and statistically large. Not one study described all 27 experimental conditions. This finding might relate to the fact that some experimental conditions—eg, the ARI and thermocycling—were not used in all studies. However, when evaluating the 121 studies for the most relevant experimental conditions, only 28 fulfilled the threshold value. This finding indicates that most of these in-vitro studies did not properly report important confounding factors that affect bond strength outcomes. When we finally included 24 of these 28 studies in a meta-analysis, water storage of the bonded specimens, photopolymerization time, and crosshead speed were shown to be the variables that primarily affected the bond strength outcomes.
Water storage decreased bond strength on average by 10.7 MPa. Although this was the most pronounced effect of an experimental condition on in-vitro bond strength outcomes, this finding was mainly influenced by 1 relatively large study sample in which artificial saliva was used as a storage medium for specimens. Most in-vitro bond strength studies used distilled water for storing the specimens, but 11% of the studies did not report the storage medium. It was previously reported that specimen storage in artificial saliva reduces bond strength similarly to the effect of water degradation. Although our study indicates that distilled water has a different effect on bond strength than artificial saliva, future research on the effects of different storage media on bond strength is needed.
The second experimental condition that we found to significantly affect in-vitro bond strength was photopolymerization time. Each additional second of photopolymerization increased bond strength by 0.077 MPa. It was previously suggested that photopolymerization time has a greater influence on in-vitro bond strength than the type of photopolymerization device. The studies in this meta-analysis showed considerable variations in photopolymerization time: from 2 to 50 seconds. Moreover, 31% of the included studies did not even report polymerization time ( Appendix ). Most remaining studies used 40 seconds for polymerizing the adhesive; this corresponds to the routine clinical standard. The fact that the majority of these studies used a halogen device for polymerizing the adhesive most likely explains why this polymerization time was used. The results from our meta-analysis, however, suggest that a longer polymerization time yields higher bond strengths, although the most optimal time for polymerizing the adhesive cannot be deduced from our results.
The third experimental condition shown to significantly affect outcomes of bond strength testing was crosshead speed. An increase in crosshead speed of 1 mm per minute yielded an increase in average bond strength of 1.3 MPa. The opposite effect was demonstrated in 2 previous studies in which increases in crosshead speed from 0.5 to 5.0 mm per minute and from 1 to 200 mm per minute, respectively, were associated with significant decreases of in-vitro bond strength. This phenomenon was suggested to relate to the induction of a stiff body response and the elimination of the viscoelastic properties of the adhesive. In another study, no effect was observed on bond strength with crosshead speed variations between 0.1 and 5 mm per minute. In the studies included in this meta-analysis, crosshead speeds ranged from 0.1 to 5 mm per minute with most using a speed of 0.5 mm per minute ( Appendix ). We have no obvious explanation for the discrepancy of our results with those of previous studies; unknown confounders might be responsible.
Bond strength values reported in the 24 studies in this meta-analysis ranged from 3.5 to 27.8 MPa. Clinical implications of in-vitro bond strength values are generally based on the recommendation in a review article from 1975 ; a “clinically acceptable” value was defined as an in-vitro bond strength of 6 to 8 MPa. According to this criterion, 53 of the 65 experimental groups from our meta-analysis should be considered to have clinically acceptable bond strength values. Because it has never actually been tested whether 6 to 8 MPa is a sufficient in-vitro bond strength for clinical use, the use of this reference value has been criticized before. Since the publication of this reference value, various materials have been used, and the effects of various test conditions (eg, pH and temperature variations) have been implicated in the aging of composite resins. This implies that interpretation of bond strength data should be limited to the relative effectiveness of the adhesives used in a study. Extrapolation of absolute values and comparing them with a supposedly “clinically acceptable” reference value should be avoided.
Since shear bond strength testing is the most commonly used method for debonding brackets, only studies that used this method were included in our review. With respect to shear bond strength testing, there are also some variations in blade design. Most studies used a shearing blade for debonding the brackets, whereas in some studies a wire loop was used. Debonding brackets with a wire loop is not a true form of shear bond strength testing, since it also incorporates a component of tensile stress. Although blade design could not be identified as an experimental condition that significantly affected in-vitro bond strength results in this meta-analysis, different shearing blades could have an effect. This should be substantiated by additional studies.
Theoretically, in-vitro studies determine the true strength of a given bonding system to the enamel substrate. Unfortunately, in-vitro studies have not been successful in predicting in-vivo effectiveness. An accurate simulation of the clinical situation seems necessary to obtain clinically relevant results from in-vitro experiments. However, because of the many conditions involved in the in-vivo situation, an accurate simulation is at present an unrealistic goal. Although in-vitro bond strength testing is valuable for initial screening and selection of materials, it cannot be regarded as a substitute for in-vivo testing. Orthodontic materials that perform well in in-vitro experiments should always be tested with in-vivo RCTs.
Although we systematically reviewed the current literature on in-vitro shear bond strength testing, our study has some possible limitations. Selection bias could have resulted in inappropriate inclusion or exclusion of studies based on factors other than the inclusion criteria. This chance was minimized by having 2 observers independently assess the articles. Another shortcoming might have been our language restriction. Moreover, only 2 databases were searched. Some relevant studies might have been missed by doing so. However, we believe that our conclusion of poor descriptions of test conditions in most in-vitro bond strength studies would not be altered by studies that were possibly missed because of language and database restrictions. This is substantiated, since 93 (77%) of the 121 potentially appropriate studies were excluded from the meta-analysis because test conditions were not adequately reported. Finally, this is a systematic review concerning in-vitro observational studies. Conclusions in systematic reviews and meta-analyses are preferably based on results from RCTs. No RCTs were available for the topic of this systematic review and meta-analysis. Selection bias, information bias, and unknown confounders threatened the validity of each study that we evaluated. In future in-vitro studies, bracket debonding should be evaluated more carefully by considering the items studied in this review. With this approach, the most dominant factor affecting bracket adhesion in vitro might also be identified and correlated with the clinical situation.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


