Introduction
Rapid palatal expanders (RPEs) have attachments cemented to the teeth and a screw that covers the palate. Because of their position and relative size, RPEs can affect speech. Our objective was to assess speech perturbation and adaptation related to RPE appliances over time.
Methods
RPEs were planned for the treatment of 22 patients in the orthodontic clinic at the University of Toronto in Canada. Speech recordings were made at 6 time points: before RPE placement, after placement, during expansion, during retention, after removal, and 4 weeks after removal. The speech recordings consisted of 35 sentences, from which 3 sentences were chosen for analysis. Speech acceptability was assessed perceptually by 10 listeners who rated each sentence on an equal-appearing interval scale. The vowel formants for /i/ and the fricative spectra for /s/ and /∫/ were measured with speech analysis software. Repeated-measures analysis of variance with post-hoc paired t tests was used for statistical analysis.
Results
When the appliance was placed, speech acceptability deteriorated. Over time, the ratings improved and returned to baseline when the appliance was removed. For the vowel /i/, the first formant increased, and the second formant decreased in frequency, indicating centralization of the vowel. The formants returned to the pretreatment levels during treatment. For the fricatives (/s/ and /∫/), low-to-high frequency ratios indicated that the fricatives were distorted when the appliance was placed. The ratios returned to baseline levels once the appliance was removed. The results for the spectral moments indicated that spectral mean decreased and skewness became more positive. Repeated-measures analysis of variance showed significant effects for time for all acoustic measures.
Conclusions
Speech was altered and distorted when the appliance was first placed. The patients’ speech gradually improved over time and returned to baseline once the appliance was removed. The results from the study will be useful for pretreatment counseling of patients and their families.
Palatal expanders such as the hyrax rapid palatal expander (RPE) are used to widen the maxillary arch. The expander’s central jackscrew and attachments stretch across the palate, and this can interfere with proper linguopalatal contact and speech sound production. However, the nature of such speech sound distortions during treatment has not been described in the literature.
The initial physical discomfort and functional impediments associated with an orthodontic appliance can affect the patient’s compliance and potentially hinder a successful outcome. Compliance and treatment success can be improved when patients are aware of potential difficulties with an appliance before treatment, and when the patient perceives an internal locus of control. In the case of RPEs, this discussion should include how long speech is likely to be affected and how the speech perturbations will play out over time.
De Felippe et al investigated the influence of palatal expanders on speech, oral comfort, swallowing, and mastication. A questionnaire was given to patients who had completed treatment with an expander before the survey. Expander types included the hyrax (banded or bonded), Haas, and quad-helix. Most patients stated that the expander affected their speech. Alveolar sounds such as /s/, /z/, /t/, and /d/ were the phonemes perceived to be the most distorted. The patients reported that the speech problems resolved by the end of the first week after appliance placement. This investigation was limited to a subjective, retrospective questionnaire and did not obtain quantitative acoustic measures of the patients’ speech.
To produce speech, the tongue interacts with the palate and alveolar ridge, which are passive structures. The passive structures are important determinants of the speech sound quality. Distortions of /s/ (lisps) might result from an anterior open bite or palatal anomalies. Dental appliances such as complete dentures, orthodontic retainers, and bite-blocks can have significant effects on consonant and vowel productions. The tongue can adapt to changes in the oral cavity within certain physiologic and functional limits. However, when speech has been distorted over a period of time, psychologic or physical factors can hamper a patient’s further adaptation. There are significant individual variations between speakers’ use of compensatory mechanisms to overcome palatal speech perturbation effects. Front high vowels such as /i/ are more likely to be affected by dental appliances. The fricatives /s/ and /∫/ are particularly sensitive to even relatively minor modifications to the anterior palate and alveolar ridge. Palatal modifications have greater effects on consonants than on vowels because consonants require more accurate positioning of the tongue.
In studies of the timeline of adaptation to an experimental palatal perturbation or a real dental appliance, speech adaptation was found to be faster and more complete for vowels than consonants. Significant palatal modifications require a long period of adaptation before the mechanical obstacle can be accommodated. Even with practice, the short-term articulatory adaptation tends to be incomplete. Patients who had childhood lisps and other articulation disorders take longer to adapt to a maxillary denture.
The position and shape of RPE appliances of the hyrax type are unique. The questionnaire study by De Felippe et al demonstrated the relevance of RPE-related speech distortions for patients. In clinical practice, orthodontists using RPEs will tend to counsel their patients that they will sound better with time. This information is typically based on clinical intuition rather than research evidence. In this study, we aimed to provide insight into the typical patterns of speech adaptation in patients wearing a hyrax RPE.
We were also interested in the 2 fixation mechanisms for the hyrax RPE. Banded expanders are fixed to the first premolars and first molars with dental bands. Bonded expanders have acrylic attachments that cover the buccal, lingual, and occlusal surfaces of the premolars and molars. It was expected that the bonded appliances would cause poorer speech outcomes than the banded variety because of an additional bite-block effect.
Material and methods
Ethics approval was granted by the Health Sciences Research Ethics Board at the University of Toronto in Canada. Based on a power calculation, it was determined that the minimum enrollment target was 15 participants. Twenty-two patients planned for treatment with an RPE in the Graduate Orthodontic Clinic at the University of Toronto were recruited for the study. Thirteen patients were female and 9 were male, with ages ranging from 9 to 19 years (mean, 14 years). The need for an RPE as part of a patient’s treatment was determined by the treating orthodontic residents and their supervisors. The study did not alter the overall orthodontic treatment and did not add extra visits for the participants. All treatment procedures, such as dental impressions, and cementation and removal of the appliances, were performed by the orthodontic resident assigned to each patient. Based on the residents’ decisions, 11 patients received banded appliances, and 11 patients received bonded appliances. In addition to the RPE, mandibular brackets on the buccal side were typically placed a few months into the treatment (during the retention phase). No participants wore concurrent appliances that involved bite-blocks or that encroached on the lingual surfaces of the teeth or the palate. A speech recording approximately 5 minutes long was made 6 times throughout treatment. All speech recordings were made by the first author (K.S.).
All 22 RPEs were made by the same laboratory technician at the Faculty of Dentistry at the University of Toronto. The RPEs were fabricated with a central jackscrew. The expander mechanism was attached to 4 extensions from the dental bands or the bonded acrylic arising from the lingual surfaces of the first premolars and molars. Although there was no standard distance from the palate to the screw and the extension arms, this distance was never less than 5 mm. The screw was not flush to the palate to prevent trauma to the palatal mucosa during expansion. For the bonded RPEs, the acrylic that attached to the teeth was approximately 2 mm thick on the occlusal, buccal, and lingual surfaces.
Fifteen sentences from the sentence module of the Fisher-Logemann test of articulation and 20 sentences from the Great Ormond Street speech assessment were used for the recordings. These sentences contain all sounds of Canadian English. All speech samples were collected by using a laptop computer with a high-quality microphone (M201; Fostex, Tokyo, Japan) and the recording software Audacity ( http://audacity.sourceforge.net/ ). All samples were recorded in a quiet room directly onto the hard disk drive by using a microphone placed 5 cm below the patient’s chin. The acoustic data were recorded with 16-bit encoding and 44.1 kHz sampling rate.
Each patient read all 35 sentences at 6 time points: just before RPE placement and cementation (TP1); within 15 minutes after RPE placement (TP2); during the RPE activation phase, typically 2 to 4 weeks after the first recording (TP3); during the RPE retention phase, typically 2 to 3 months after the first recording (TP4); after the RPE was removed, typically 5 to 6 months after the first recording (TP5); and 1 to 2 months after the RPE was removed, typically 6 to 8 months after the first recording (TP6).
Based on the observations by De Felippe et al, the analysis was limited to speech sounds that are known to be particularly affected by a palatal expander. From the 35 sentences that were recorded, 3 were selected for analysis in this study. The sentence, “Let me keep a little of this wedding cake to eat later,” was selected to assess the impact of the appliance on the high front vowel /i/. “Suzie sewed zippers on 2 new dresses at Bessie’s house” was used to assess /s/, and “Sean is washing a dirty dish” was used to analyze /∫/.
Speech acceptability was assessed by 10 naïve listeners (5 men, 5 women), who evaluated the 3 sentences of the 22 patients at all 6 times. The participants were undergraduate students who were unaware of the purposes of the investigation and had no prior training in phonetics, linguistics, or dentistry. The recordings were blocked and randomized for the presentation. The participants listened via headphones (1210; Telex Communications, Burnsville, Minn) to all 396 recordings at a comfortable loudness level and graded the patients’ speech with a 4-point equal-appearing interval scale, as follows: 0, normal speech acceptability; 1, speech acceptability mildly affected ; 2, speech acceptability moderately affected; and 3, speech accpetability severely affected.
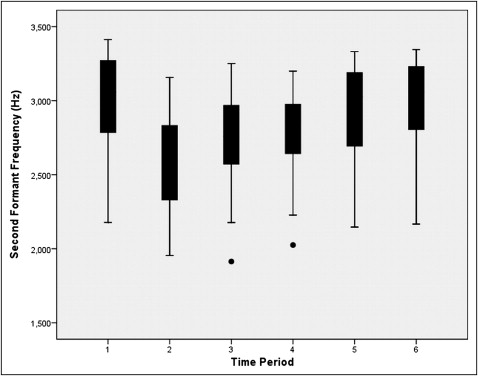
By using WaveSurfer software (version 1.8.5), acoustic analyses were completed for 2 tokens of the vowel /i/ from the sentence, “Let me keep a little of this wedding cake to eat later.” The /i/ sounds of the words “keep” and “eat” were segmented for speech analysis. Long-term linear predictive coding (512 points; Hamming window) was used to measure the first (F1) and second (F2) formants at each time for each patient. Formants are regions of high acoustic energy and are measured as an amplitude peak in the frequency spectrum. The patients were of different ages and sexes, which are factors known to influence formant measurements. Therefore, a relative measure to define the distance between the 2 formants was calculated. The distance between F1 and F2 was measured, and a ratio was calculated by dividing this distance for each time period by the distance at TP1.
By using the WaveSurfer software, acoustic analyses were completed for the phonemes /s/ and /∫/. The /s/ sounds from the words “dress,” “Bessie,” and “house” were segmented from the sentence “Suzie sewed zippers on 2 new dresses at Bessie’s house.” The /∫/ sounds from the words “washing” and “dish” were taken from the sentence “Sean is washing a dirty dish.” Long-term fast Fourier transformations (64 points; Hamming window) were used to evaluate the spectral features of each fricative. The output for each phoneme consisted of uncalibrated amplitude values in decibels for 32 frequency bands. Since the amplitude values were not calibrated, a ratio of the amplitude associated with a low frequency band divided by the amplitude associated with a higher frequency band was calculated. This ratio described the crispness or acoustic clarity of the fricative. The associated volume of the peak was expected to be attenuated with the placement of the RPE. Because the decibel values obtained were all negative, a lower ratio value indicated less acoustic clarity of the fricative sound.
The spectral peak for /s/ is usually in the 3500 to 5000 Hz range. The amplitude associated with the frequency band of 4125 Hz was selected as the higher frequency in the calculation of the ratio for /s/. The amplitude associated with the frequency band at 1625 Hz was chosen as the numerator. The decibel ratio of the amplitudes at 1625 Hz divided by the amplitude at 4125 Hz was used for the statistical analysis of /s/.
The major spectral peak for /∫/ is observed in the 2500 to 3500 Hz range. By using similar criteria as for the /s/ ratio, the decibel ratio of the frequency bands at 875 and 3125 Hz was used in the statistical analysis of the /∫/ sound.
The spectral moments for the fricatives /s/ and /∫/ were also calculated. The 4 moments summarized the concentration (mean), variance (standard deviation), tilt (skewness), and peakedness (kurtosis) of the energy distributions. Using the Kay Elemetrics Multi-Speech device (model 3700; KayPentax, Lincoln Park, NJ), the recordings were low-pass filtered to 11.025 kHz, following the procedure used by Forrest et al and Jongman et al. Fast Fourier transformations were calculated using Hamming windows with 98% preemphasis. Spectral moments for each fricative were calculated with a 40-ms Hamming window at the central 40-ms location. For each phoneme in the sentence, the spectral mean, standard deviation, skewness, and kurtosis were measured.
Statistical analysis
Average acceptability ratings were calculated for the 10 listeners for each recording. For the acoustic data for each sound at each time, histograms were created to examine the data distributions. The data sets were all normally distributed.
To investigate whether patients with preexisting speech difficulties had additional issues adapting to the RPE, the TP1 average ratings for the 22 patients were examined. The 22 participants were placed into 2 groups: normal and preexisting speech difficulties (PESD). The 12 patients with average ratings of less than 0.7 (least speech distortion) were the normal group, and the 10 patients with ratings of 0.7 or greater were the PESD group. The average ratings for the PESD group ranged from 0.7 to 2.2. This normal or PESD variable was used when analyzing the acceptability data and also for each of the 3 phonemes examined in this study.
The statistical analyses were conducted by using repeated-measures analysis of variance (ANOVA) with post-hoc paired t tests or independent t tests. Box plots were used to examine the interactions between the variables. Missing data for individual patients were replaced with the group mean. No Bonferroni adjustments were made, in keeping with the recommendations of Perneger.
Results
The listeners’ average ratings of the 3 sentences for each of the 6 times showed that, at TP2, the patients’ speech acceptability scores increased (speech acceptability deteriorated). Over time, the acceptability scores decreased (speech acceptability improved), only returning to TP1 levels at TP5. At TP6, the scores were decreased compared with the TP1 levels (speech acceptability improved). Figure 1 is a graphic representation of the results.
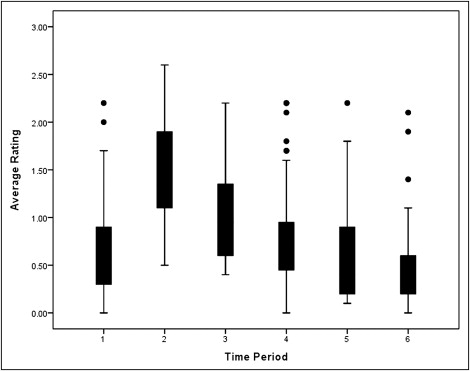
Repeated-measures ANOVA was performed to examine the average ratings with respect to time period and whether appliance type (banded or bonded RPE) or the TP1 speech rating (normal or PESD) influenced the results. The effect of time period was significant ( P <0.001; 1 − β = 1; ηp 2 = 0.633; df = 5, and F = 84.372). Post-hoc analyses of time period with paired t tests showed significant differences between all pairs ( P <0.05) except TP1 and TP5.
No significant differences were found between the normal and PESD patients, or between the banded and bonded appliance types.
From the sentence, “Let me keep a little of this wedding cake to eat later,” 2 tokens of /i/ were analyzed: “keep” and “eat.” At TP2, the F2 decreased, and the F1 increased. Over time, both formants began returning to the TP1 level (F2 increased, and F1 decreased). By TP4, the F1 reached its TP1 level, whereas the F2 only returned to the TP1 level at TP6. Figures 2 and 3 illustrate the results.