Fig. 20.1
Oscar Amoëdo‘s book in German translation by Gottlieb Port (1900)
Forensic odontologists of 27 national societies founded the International Organisation for Forensic Odontostomatology (IOFOS) in Paris (1973) and another 23 societies are associated. In Germany, an interdisciplinary working group of forensic odontostomatology, the German Academy of Forensic Odontostomatology (founded 1976) is a member of the IOFOS.
In various areas of forensic disciplines, the teeth are significant indicators used for age estimation and sex determination because of their individual character. The main application of forensic odontostomatology is the identification of victims in the wake of disasters and crimes (Alt 1997a; Alt et al. 1995; Alt and Türp 1998; Alt and Vach 1995). It is part of a multidisciplinary complex of identification methods.
Among the most spectacular odontological identifications in recent German history is the identification of Adolf Hitler, who was Chancellor from 30 January 1933 to 30 April 1945, when he committed suicide in the bunker of the Reich Chancellery with his wife, Eva Braun, and Martin Bormann, his secretary. Adolf Hitler and Eva Braun were identified beyond doubt by their dental status, while the identity of Martin Bormann could only be confirmed by mitochondrial DNA analysis (Rötzscher 1998a).
Their identification is based on documents from Soviet and American archives, photographs (Fig. 20.2), diagrams, descriptions (interrogations), and skull X-rays (US National Arch and Rec Services: APO 757, 01-FIR/31). Five X-rays of Adolf Hitler were used to identify his odontological status (Figs. 20.3 and 20.4). The X-ray image was taken on 19 September 1944 (Fig. 20.5) after the failed assassination attempt of 20 July 1944.

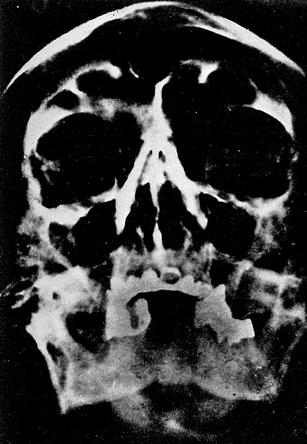
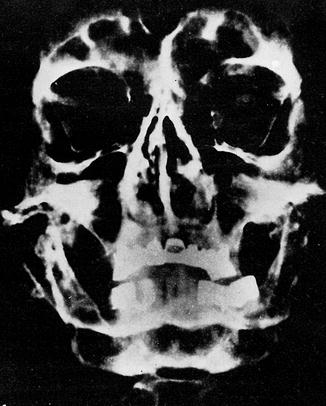
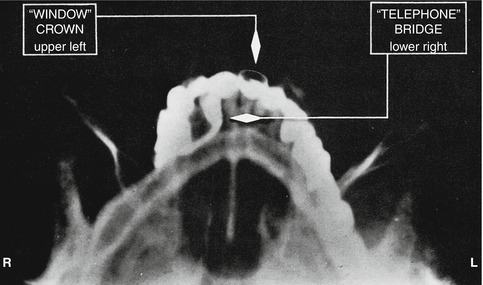
Fig. 20.2
Adolf Hitler: Lingual view of mandibular incisors and the right quadrant, with the characteristic lingual bridging of the intact first premolar (Sognnaes and Strøm 1973) (Courtesy of Dr. Michel Perrier, Lausanne, Switzerland)
Fig. 20.3
Skull X-rays of Hitler from 21 October 1944
Fig. 20.4
Chin–nose projection of Hitler (Courtesy of Dr. R. F. Sognnaes, Dr. F. Strøm, Prof. Dr. T. Solheim, Oslo, Norway, and Dr. Michel Perrier, Lausanne, Switzerland)
Fig. 20.5
Jaw X-ray of Hitler with extensive crown and bridge work of unusual construction (Courtesy of W. B. Saunders Company, Philadelphia, PA, USA)
20.1.1 The Identification of Adolf Hitler
Berlin-Buch, 8 May 1945, Army Surgical Hospital morgue, Nr. 496.
Thirteen bodies were examined (Sognnaes and Strøm 1973). Bodies no. 12 and 13 were the most demolished by fire. A commission of five medical experts, army anatomists, forensic experts, and pathology anatomists of the First White Russian Front, the Red Army, and the 3rd Shock Army examined, by order of the Military Council of the First White Russian Front, the male body (presumably Hitler’s body).
Act No. 12 is the forensic examination of a burnt male body (probably Hitler’s body) (documents from Moscow archives) (Bezymenski 1968). The corpse is badly burnt. A portion of the skull is missing. Parts of the occipital bone, the left temporal bone, the lower parts of the cheek and nasal bone and the upper and lower jaw are preserved. The nose and the upper jaw bone show many small fractures. The tongue is burnt, the tip of the tongue firmly stuck between the teeth of the upper and lower jaw.
Sognnaes compared the final report (Soviet Army Surgeon) of the dental status with the details of the dentist Blaschke and his own list compiled in 1975. Sognnaes and Strøm (1973) graphically presented the dental status of Hitler (Fig. 20.6).
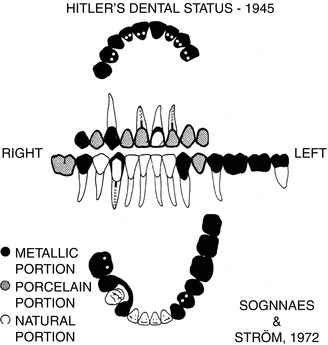
Fig. 20.6
Dental status of Hitler (drawing) at time of death (Courtesy of Sognnaes and Strøm 1973)
The record of the hearing of Käthe Heusermann (assistant of Dr. Hugo Johannes Blaschke) confirms the assumption that the described teeth and bridges are assigned to Hitler. In a meeting with the chief forensic expert, Lieutenant Colonel Shkaranskij, on 11 May 1945 in the premises of CAFS Nr. 496 (see above), Heusermann and Echtermann, the dental technician, described in detail the condition of Hitler’s teeth.
20.1.2 The Identification of Eva Braun
Act No. 13 is of the forensic examination of a burnt female body (probably Eva Braun) (Bezymenski 1968):
Protocol No. 13: Results of the forensic examination of a female body: Yellow glass fragments of a thin-walled ampoule were found in the mouth. The death was a result of poisoning with Cyanide. The most important anatomic findings were the gold bridge of the mandible and the outer four teeth.
Gorbushin (assistant of the chief of the 3rd Army) stated:
The evidence to establish the identity of the bodies should be sought due to medical recommendations. In the clinic of Prof. Blaschke, we were welcome by Dr. Bruck. As Bruck learned that we wanted to talk to Prof. Blaschke because of an identification matter, we were told that Professor Blaschke is not in. Mrs. Heusermann handed me the medical history of Adolf Hitler. The X-ray images of Hitler’s teeth were supposed to be in the office of Prof. Blaschke in the Chancellery. We found them in the basement of the dental treatment room by help of Mrs. Heusermann. We also detected several gold cups for Adolf Hitler. Käthe Heusermann informed me that crowns and bridges for Hitler and Eva Braun were made by the dental technician Fritz Echtmann. We met him at his home. His information about the bridges, crowns and fillings exactly corresponded with the medical history and X-ray images. Then Mrs. Heusermann and Mr. Echtmann were submitted for identification of the jaw bone of the male body. They both identified it as Adolf Hitler’s.Then we asked Mrs. Heusermann and the dental technician Fritz Echtman to describe the teeth of Eva Braun. We showed them the gold bridge we found in the female body. Fritz Echtermann added that the unique design is the bridge made for Eva Braun. The experts came to the final conclusion that these teeth belong to Eva Braun.
20.1.3 The Identification of Martin Bormann
On 7 and 8 December 1972, during excavation work near the Weidendamm bridge at Lehrter Subway station (Berlin), two relatively well-preserved skeletons (Martin Bormann and Dr. Ludwig Stumpfegger?) were found (Figs. 20.7 and 20.8). Later, some teeth and a gold dental bridge were found (Fig. 20.9). There were uncertainties concerning the identification of one of the bodies, because no X-ray images of Martin Bormann existed, only a dental chart by Prof. Blaschke, drawn from memory in 1945. Prof. Blaschke had been Bormann’s dentist (1937–1945) (Fig. 20.10).
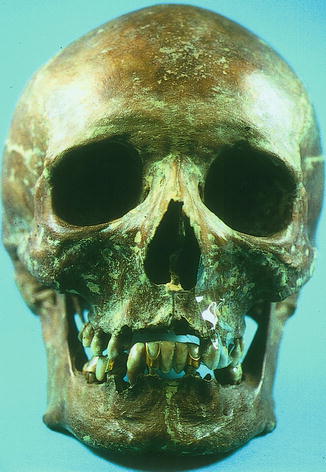


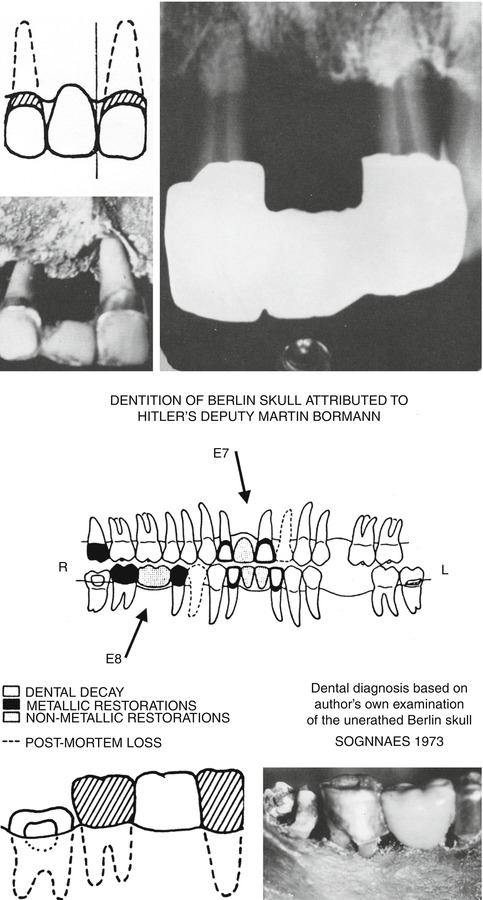
Fig. 20.7
Martin Bormann, a front shot of the skull
Fig. 20.8
Skull and mandible with a gold bridge on the right (Courtesy of Prof. Dr. W. Eisenmenger, Institute of Legal Medicine, University Munich. Released for publication by the public prosecutor in Frankfurt/Main, December 1999)
Fig. 20.9
Maxillary anterior bridge (teeth 12–21), no longer located in the jaw (Courtesy of Prof. Dr. W. Eisenmenger, Institute of Legal Medicine, University Munich. Released for publication by the public prosecutor in Frankfurt/Main, December 1999)
Fig. 20.10
Antemortem drawing by Dr. Blaschke. Bormann’s maxillary bridge and mandibular bridge (see arrow) (Courtesy of W. B. Saunders Company, Philadelphia, PA, USA)
Prof. Dr. Wolfgang Eisenmenger, Director of the Institute, and Mrs. Dipl.-Biol. Katja Anslinger of the Institute of Legal Medicine, Ludwig-Maximilians-University, Munich, confirmed the positive identification of Martin Bormann with a mitochondrial DNA analysis from femurs and tibias only in 1998; two approximately 5-g bone pieces were extracted from each for the analysis. All four bone samples identically matched with mtDNA sequences of two blood samples of a family member of Martin Borman. This proves, together with all other findings, that the skeletal parts are Martin Bormann’s (time of death: early morning hours of 2 May 1945).
Dr. Johannes Hugo Blaschke, a graduate of the University of Pennsylvania (1911), was owner of a dental practice in Berlin Kurfürstendamm and became Hitler’s dentist (1934–1945). After his capture in 1945, in the headquarters of the US Armed Forces in Europe, Military Intelligence Service Center, APO customized-757, he recorded the medical history of Hitler (Final Interrogation Report [OI FIR/31, 1946]). Another document contains information about the dentition of Eva Braun and Martin Bormann (Sognnaes and Strøm 1973). One of his first patients was Hermann Goering. Soon after, the “elite” of the Third Reich was his clientele.
A systematic interdisciplinary cooperation between the investigating authorities and the medical (anthropologists, biologists, radiologists, forensic medicine, serological) and dental experts (forensic odontologists) is required for a thorough identification. In particular, identification after fires, mining accidents, and plane crashes is accelerated or even made possible by dentition features. Furthermore, teeth are very resistant to external influences (Rötzscher 1971). Every rescue identification unit should include at least one forensically trained dentist, ideally already a part of the unit at the time of the incident (Benthaus and Endris 1999; Dittmer and Dumser 1999).
Possibilities of registration of dental findings according to Fiala (1968) are shown in Chart 20.1. An intact dentition shows many specific points of comparison. However, treatment records must be available for comparison. Without those records, an identification can take weeks or months. The military has recognized the value of current and accurate premortal dental status records, which must be accessible in a very short time. In civilian life, many companies that are afflicted with a high risk for accidents, such as airline companies, strictly require dental findings, including color photographs of their staff (Fig. 20.11) (Johanson and Lindenstam 1961).
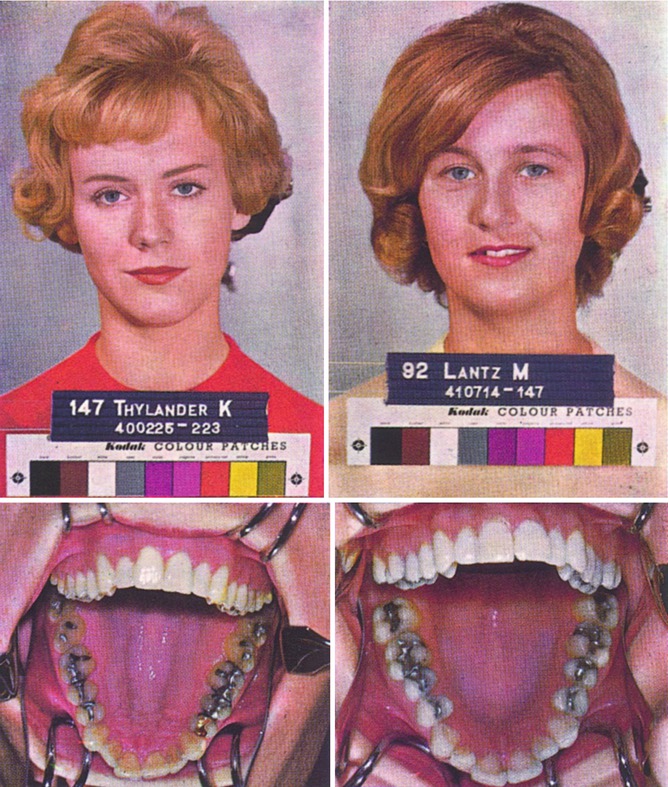
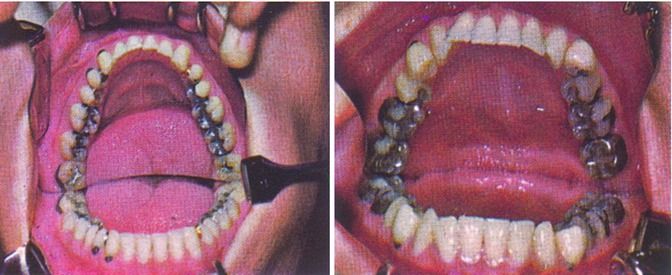
Fig. 20.11
Color photo, part of registration of airline personnel in Sweden (Courtesy of Prof. Dr. G. Johanson, Malmo, Sweden)
Chart 20.1
In cases of flight accidents, it is much easier to identify the bodies of military or airline personnel because of the accessibility and accuracy of their dental records (Johanson and Lindenstam 1961). The investigative reports of dentists and their index cards (records), together with dental charts and X-ray images, are the most valuable indicators. If possible, a forensically experienced dentist should be consulted (Schneider and Wandelt 1984).
In determining the identity of an unknown or unrecognizable dead, the findings of the teeth and jaws are one of the most efficient methods. All surveys should preferably be fixed in the treatment card and in a dental chart (Rötzscher 1991, 1995). The identification of living/dead on the basis of dental status is often complicated by incomplete treatment records. Many dental practices neglect the recording of the initial examination and only record their own treatments (see Sects. 18.1 and 18.2).
20.2 Gender
(3)
German Academy of Forensic Odontostomatology (AKFOS), Wimphelingstraße 7, 67346 Speyer, Germany
(4)
Institute of Legal Medicine, Turmweg 22, Leipzig, 04277, Germany
20.2.1 Odontometric Gender Determination
Skeleton parts that are useful for gender determination often are incomplete or poorly preserved. Therefore, teeth are particularly suitable for accurate and repeatable measurements. For these reasons, morphognostic and metric studies of gender characteristics are of high value (Albus 1998). Regarding the doctrine from 1964 that a gender determination by the aid of teeth and dentures is not possible (sexual dimorphism) or very doubtful (Schranz and Bartha 1964), recent studies have proven the opposite (Pilz 1974; Pilz and Krause 1980b).
Studies of front teeth by Schranz and Bartha (1964) showed that the crown width in males often, but not always, is larger than in females (Fig. 20.12). In female subjects, 2.42 % aplasia or hypoplasia of the maxillary lateral incisor was found, in males, it was only 0.58 %. Hyperodontia, mesiodens, gemination of the central incisors, two lateral incisors, three premolars, and four molars predominantly occurred in males. Both jaw halves must be examined and the findings must be completed by X-ray images. Radiographic studies showed that bifurcated roots of the lower first premolars occur twice as often (26.66 %) in males than in females (11.43 %) (Table 20.1).
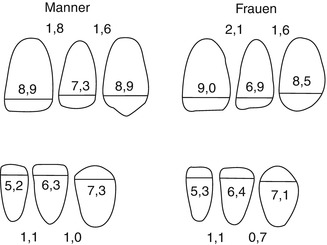
Fig. 20.12
Cross-average of upper and lower front teeth (Schranz and Bartha 1964)
Table 20.1
Comparison of the particulars of the female and male dental morphological type with regard to gender characteristics (Schranz and Bartha 1964)
|
Female
|
Male
|
|---|---|
|
1. Minimum transverse diameter values exclusively in females
|
1. Maximum transverse diameter values are not gender dependent
|
|
2. The upper central incisor is wider than the canine
|
2. The upper central incisor and the canine have the same width
|
|
3. The difference in width between the upper central and lateral incisor is larger (2.1 mm)
|
3. The difference in width between the upper central and the lateral incisor is larger (2.1 mm)
|
|
4. The difference in width between the lower incisor and canine side is smaller (0.7 mm)
|
4. The difference in width between the middle incisor and the canine is bigger (1.0 mm)
|
|
5. Fusion of the roots of the lower 12-year molar is more common (30.9 %)
|
5. Fusion of the roots of the bottom 12-year molar is rare (22.0 %)
|
|
6. Aplasia (hypoplasia) of the teeth is more common
|
6. Supernumerary teeth (hyperodontia) are more common
|
|
7. The wisdom tooth often is missing
|
7. The wisdom tooth is missing less often
|
Today, odontometric gender determination is an important feature for the identification of unknown skeleton remains as well as the treatment of skeleton remains from archaeological excavations. A detailed literature review on the research and method development about sexual dimorphism is presented by Albus (1998). Teeth currently provide the only basis for gender determination of children and adolescents (Reuling 1992). Preferred starting points are measurements of the crown diameter. Their mean values in boys are higher than in girls (Moorrees et al. 1963). Previous studies showed that sexual dimorphism in the deciduous dentition is significantly present, but less than in the permanent dentition. In 1978, for the first time, Black applied discriminant analysis of milk teeth for gender determination (he evaluated 64 white girls and 69 white boys from Ohio). His hit rate was relatively low (63.9–67.7 %). Other researchers also studied the permanent teeth and attained much better results. evaluated 109 white boys and 95 white girls, with a hit rate of 86 %.
The single features of the teeth are not very significant in terms of gender specifics. Taken together with the indicators of the general skull and the mandible, the value of the dental characteristics for determination increases (Albus 1998). Gender determination by the quantitative analysis of the tooth width has gained a strong appreciation in recent years by applying the discriminant method (Alt and Vach 1995; Alt et al. 1995; Pfeiffer 1989, 1990; Starp 1990; Teschler-Nicola 1992).
New methods have also been developed for single teeth (Rao et al. 1989) and for the characteristics of the mandible (Pötsch-Schneider et al. 1985). Correlation analysis shows individual relationships between the widths of permanent teeth, i.e., in homologous neighboring teeth (central and lateral incisor, first and second premolar/molar) and the homologous antagonist (e.g., upper and lower right canine). In most cases, the gender determination was confirmed by the teeth sizes.
The canines are more resistant to periodontal disease and even to severe trauma than other teeth, and may therefore be best used to identify a person. Rao et al. (1989) propose a technique that is based on the evaluation of the Mandibular Canine Index (MCI), the relationship between two parameters of the permanent lower canine.
The mesiodistal crown diameter (MDKD) and the width of the canine–mandibular arch (WCMB) in millimeters is:
The mean MCI value is 0.296 (±0.016) for the male and 0.254 (±0.014) for the female gender. There is a significant difference between them.
The result is the standard value:

All values above the standard characterize the female gender; all values under the standard characterize the male gender. The accuracy of the MCI method is 84.3 % in males and 87.5 % in females. The authors note that a more accurate assessment can only be made after further tests regarding the characteristics of the studied population.
The sole use of tooth size for gender diagnosis is limited and should only be applied in cases where other methods, such as chromatin examination or fluorescence of the Y chromosome from the pulp cells, are not possible (Seno and Ishizu 1973).
20.2.1.1 Gender Determination Including the Jaws
In recent years, a discriminant analysis on the basis of osteometrical findings of the mandible was conducted on bodies of American, Egyptian, German, and Japanese origin.
Studies on adults of both genders in Leipzig provided significant gender differences in the:
-
Length of the mandible
-
Width of the condyles
-
Mandible angle
-
Branch width
-
Chin height
-
Branch height
-
Height of the corpus mandibulae
These results were confirmed in teleradiographs of chin height, branch height, and the height of the corpus in living adults (Leopold et al. 1988). In particular, the mandible can be used for gender determination. However, the ethnic origin must be respected. The separation function of a discriminant analysis provides good results (Pfeiffer 1990); only three variables allow a significant determination:
-
Angular width
-
Branch height
-
Height of the mandibular foramen:
The use of process analyses of complex three-dimensional structures, such as the examination of the palate and canines using “moiré topography” study (Takei 1985), will increase. The mesio-distal and bucco-lingual crown diameters are the most important parameters for odontometric investigation (Alt et al. 1995; Alt and Vach 1995).
One problem of tooth width measurements is differences between left and right sides. Opposite teeth of a jaw are approximately equal. The analysis of the data was performed using univariate statistical methods. The arithmetic mean value, the standard deviation, and the coefficient of variation of each tooth diameter, separated by gender, were determined. Almost all mean values of females are below those of males; the differences are between 0.64 mm OKBL3 (upper jaw width-length canine) and −0.3 mm OKMD8 (upper jaw-mesio-distal-tooth 8). The differences in the canines are particularly significant.
The method of discriminant analysis is an obvious choice. The principle of discriminant analysis is based on the selection of an optimal set of variables, i.e., a combination of features that ensures a maximum degree of separation between the sexes and the indication of a rule based on these variables, which allows a gender determination (Table 20.2). The assessment of the discriminant value requires mathematical knowledge (Langenscheidt 1983; van Vark 1976).
Table 20.2
Discriminant analysis to determine the gender of the mandible
|
Size (in cm)
|
Coefficient
|
|---|---|
|
Branch height
|
0.9382
|
|
Angular width
|
1.025
|
|
Height of the foramen mandibulae
|
1.087
|
|
Mean value in males
|
1.946
|
|
Cut point
|
1.8375
|
|
Mean value in females
|
1.729
|
20.2.2 Morphological Relatedness
The need for interdisciplinary cooperation between forensic medicine, forensic odontology, and anthropology is is undisputed. In addition to dental charts, morphological tooth characteristics (such as accessory cusp/roots), and dental anomalies (such as congenital aplasia of teeth), familial comparisons (kinship analysis) may provide important additional information. Genetic aspects are of great value for the consideration of the development processes of the tooth, jaw, and face area. Teeth primarily are polygenic inheritance, with modifying exogenous factors. In order to examine the genetic and environmental influence on a characteristic, an estimation of the heritability by twin, family, and kinship studies can be made (Alt 1997b; Schulze 1982). For the affinity analysis, 137 dental characteristics, divided into 15 groups, were examined (Alt 1997b).
Basically, there are four types of characteristics:
1.
Variations of the tooth crown and root
2.
Odontogenic disturbances of the form, number, size, structure, and function
3.
Selected and well-known irregular skull and jaw features
4.
Congenital anomalies and syndromes of jaw and teeth
If dental records are not available, the comparison of tooth morphologic features can be a reliable contribution (Alt et al. 1995; Alt and Türp 1998; Alt and Vach 1995).
Gender in bodies or juvenile skeletons can be determined relatively easy with molecular genetic methods. A gender determination can be performed by amplification of a segment of the XY homologous gene Amelogenin and with fast and quantitative DNA testing. Using a single primer pair that spans a portion of the first intron, PCR products of 106 and 112 bp were generated (Mannucci et al. 1994) by the homologous portions of the X and Y chromosomes, which were separated using agarose gel electrophoresis. This test made it possible for even quantities as small as 20 pg of DNA amplified from degraded bones to be typed in a single reaction.
Because of the use of dye-labeled primers, it was also possible to quantify the relative yield of X- and Y-specific PCR products by automated fluorescence detection. The versatility of this assay was also demonstrated by the fact that a co-amplification with the HLA-DQA1 “Amplitype” kit in a combined sex determination and identification DNA test was possible (Mannucci et al. 1994).
20.2.3 Palatoscopy
Planning models, impressions for dentures, orthodontics, etc. are accurate representations of a patient’s teeth and and invaluable for comparison with postmortem remains. Even models of edentulous patients (for complete dentures) can be compared postmortem with remains, such as the contour of the alveolar ridge, size, and configuration of the palatal folds (rugae palatal). Rugae are irregular ridges in the hard palate of the maxillary mucosa behind the incisors (Fig. 20.13). Wutzler and Leopold (1995) distinguish the rugae according to the anatomical location toward the median palatine raphe (Table 20.3). The average length of the main folds in women are 11.7 mm (right side) and 12.3 mm (left side). The range of variation (Table 20.4) varies between 7.2 mm (men) and 6.6 mm (women) and 22 mm. In the left half of the palate, the extra folds are a little shorter, the average value is 14 mm (Wutzler 1991). The characteristics of the face are significant, because their shape is inseparable from the bony substructure, such as the maxillary complex, with the palate. Although the anatomy and histology of the palatal folds are known, measurements of gender-specific height and width development are not available (Brückner 1993; Wutzler 1991; Wutzler and Leopold 1995). The palatal vault is divided into four categories (Fig. 20.14) (Brückner 1995).
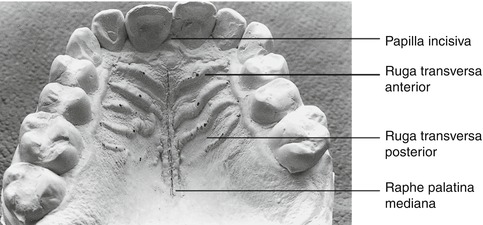
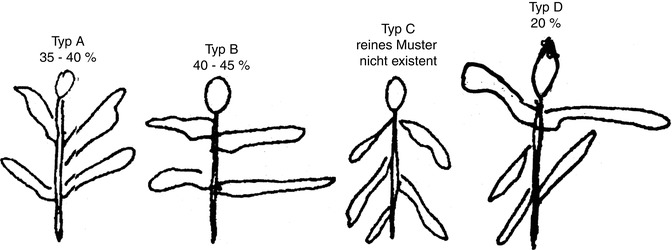
Fig. 20.13
Model with median palatine raphe and the medium and vertices marked (Wutzler 1991)
Table 20.3
Division of the existing rugae to their anatomical location for the median palatine raphe (Wutzler and Leopold 1995)
|
Main fold
|
Extra fold
|
Additional fold
|
|
|---|---|---|---|
|
Beginning
|
of raphe
|
of raphe
|
|
|
Length (mm)
|
12
|
14
|
8
|
|
Height (mm)
|
0.6
|
0.5
|
0.2
|
Table 20.4
The gender difference (average) in millimeters, statistically significant, probability of error 1 % (Wutzler 1991)
|
Extra palatal fold
|
Side palatal fold
|
Range of variation
|
|||
|---|---|---|---|---|---|
|
Male
|
Female
|
Male
|
Female
|
Male
|
Female
|
|
15.1
|
12.9
|
8.8
|
8.2
|
3–16.5
|
3–14
|
Fig. 20.14
Classification of the palatal vault (Brückner 1993)
The average number of folds on the palate relief is four for both sexes, with a maximum of seven folds in individual cases. Of all examined subjects, 50 % had a side fold, and 30 % had an extra fold. The fold curve is very different and also very variable within the age groups. The basic pattern type, according to Murakami (1931), was modified and rescaled (Wutzler 1991). If <100 %, but at least >75 % of all folds have the same direction, it is the basic type A1, B1, C1. If at least 50 % of the folds but <75 % have the same direction, it is the basic type A2, B2, C2.
20.2.3.1 Gender Differences
1.
Males have higher overall folding, main folds on two sides, wider and more frequently fragments, and more frequently have papillary folds
2.
Major folds in males are only higher at the left side
3.
Males often have three major folds at the left side
4.
Females have an even more progressive form of the folds at the left
5.
The feature “branching” at the left is significantly more common in men
6.
The extra folds at the right in males are longer and the major and minor folds are significantly wider
Most common on the level:
-
Parabolic, 38 %
-
Keystone (horizontal), 42 %
-
Concave increase (longitudinal), 46 %
Top view supervision, cross crossways:
-
Arched, trapezoid, 15 %
-
Parabolic, trapezoid, 14 %
And in three levels:
1.
Parabolic-Romanesque arch-concave increase of 3.9 %
2.
Least often: horseshoe, 25 %
3.
Gothic arch (horizontal), 23 %
Convex increase (longitudinal) and 21 % for supervision and cross gothic/horseshoe-Roman and 5 % each in three levels:
-
Horseshoe-Romanesque arch: 0.38 %
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


