Human immunodeficiency virus and acquired immune deficiency syndrome
Publisher Summary
Infection with human immunodeficiency virus (HIV) is probably the most lethal infection which can be contracted via parenteral routes. This is because the scientific community has not yet developed an antiviral agent or a vaccine which successfully combats the virus. Although the theoretical possibility of contracting hepatitis B in the dental clinic is far greater than that of acquired immune deficiency syndrome (AIDS), this is counterbalanced by the very high mortality and, indeed, the stigma and social consequences associated with the latter. These, together with the extensive media coverage and intense public awareness of AIDS, mean that the average patient would probably be more concerned about contracting AIDS than hepatitis B. Therefore, the dental practitioner should be knowledgeable on AIDS, firstly to diagnose patients who may present to him with early signs and symptoms of the disease, secondly to implement appropriate infection control measures and finally to educate, advise and allay the public fears concerning AIDS transmission both within and outwith the dental clinic environment.
Epidemiology
The main risk groups for AIDS include sexually active male homosexuals and bisexuals, recipients of blood transfusions or products, and intravenous drug abusers. In the African continent men and women are equally affected, as opposed to fewer than 10% of female patients in the UK and USA. AIDS in Africa is spreading rapidly and is often characterized by a wasting syndrome termed ‘slim disease’. Paediatric AIDS is seen in a significant proportion of infants born to infected mothers or those who received contaminated transfusions. The high risk groups for AIDS and AIDS-related diseases are shown in Table 16.1.
Table 16.1
Major risk groups for AIDS and related diseases
Sexually promiscuous homosexual or bisexual men
Intravenous drug abusers who share injection equipment
Haemophiliacs and other recipients of unscreened blood or blood products
Sexual partners of the above groups or infected persons
Infants born to infected mothers
Human immunodeficiency virus
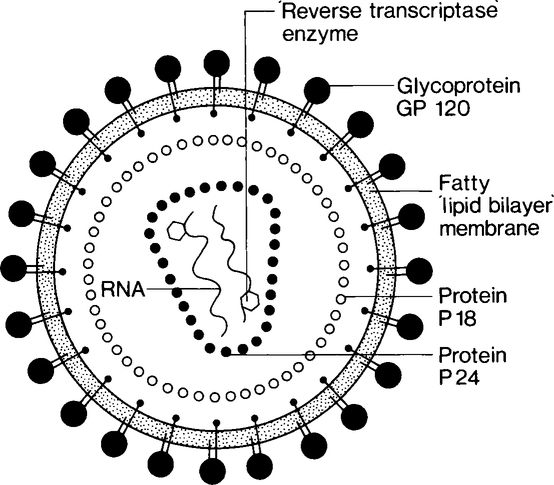
The human immunodeficiency virus has a genome of RNA surrounded by two layers of protein (P24 and P18). These layers are in turn covered by a lipoprotein layer which has glycoproteins embedded in it as ‘knob-like’ structures (Figure 16.1). Along with the RNA are molecules of an enzyme, reverse transcriptase, which the virus uses during multiplication.
Natural history and clinical features of AIDS
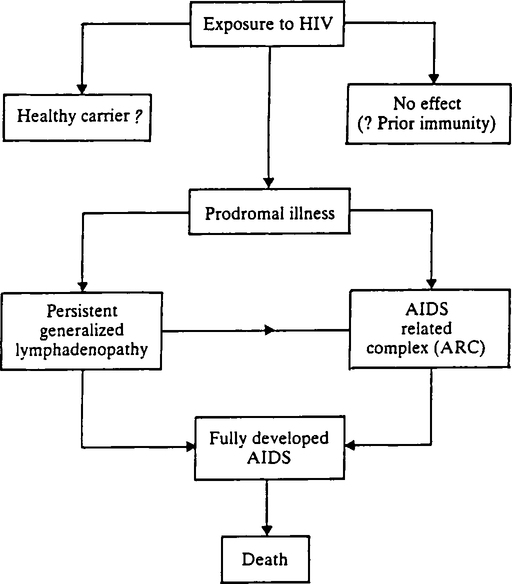
AIDS is an insidious disease process with protean manifestations. Consequently a number of stages in the natural history of AIDS has been identified, ranging from subclinical infection, persistent generalized lymphadenopathy (PGL), AIDS-related complex, and full-blown AIDS (Figure 16.2). The most common syndrome of AIDS is PGL which is due to reactive hyperplasia of lymph nodes.
The opportunistic infections, neoplasms and other features of AIDS and its prodrome are listed in Table 16.2. However, by far the most common of these opportunistic infections, seen in 50% of AIDS patients, is Pneumocystis carinii pneumonia, while the most common neoplasm is Kaposi’s sarcoma. As HIV is neurotrophic, up to 60% of full-blown AIDS patients may have clinical manifestations of encephalopathy, including dementia and paralysis.
Table 16.2
Opportunistic infections, neoplasms and other features of AIDS and related diseases
| Opportunistic infections | |
| Pneumonia, sinusitis: | Pneumocystis carinii |
| Aspergillosis | |
| Candidosis | |
| Cryptococcosis |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


