Introduction
The purpose of this study was to determine the arch form of the root apices of normally erupting teeth and then determine the differences in the location of the apex of impacted canines relative to normally erupting canines. In addition, we sought to determine whether the labiopalatal position of the impacted canines influences the position of the apices.
Methods
The study included 21 patients with unerupted canines that subsequently had a normal eruption, 21 patients with palatally impacted canines, 27 patients with labially impacted canines, and 17 patients with midalveolus impacted canines. Images were obtained using cone beam computed tomography, and the x, y, and z coordinates of the root apices were determined using Ondemand3D software (Cybermed Co., Seoul, Korea). Two-dimensional coordinates were converted from acquired 3-dimensional coordinates via projection on a palatal plane, and the Procrustes method was used to process the converted 2-dimensional coordinates and to draw the arch forms of the root apices. Finally, we measured the extent of root apex deviation from the arch forms of the root apices.
Results
Normally erupting canines showed that even though calcifications may be immature, their positions were aligned with a normal arch form. The root apices of the impacted canines were an average of 6.572 mm away from the root apices’ arch form, whereas those of the contralateral nonimpacted canines were an average distance of 2.221 mm away, a statistically significant difference. The palatally impacted canines’ root apices distribution tended toward the first premolar root apices.
Conclusions
Incompletely calcified, unerupted teeth with a subsequent normal eruption showed a normal arch form of the root apices. The root apices of impacted canines were farther from the arch forms than were the nonimpacted canines. Also, the root apices of impacted canines in the palatal area showed distributions different from those of the other impacted canine groups.
Highlights
- •
The root apex arch form was acquired from CBCT for unilateral canine impaction.
- •
The root apices of the impacted canines were an average of 6.6 mm from the arch form.
- •
The root apices of the nonimpacted canines were farther away than those on the impacted side.
- •
The root apices of the palatally impacted canines tended more toward that of the first premolar.
Maxillary canines play an important role in determining the arrangement and stability of the dentition, while also maintaining esthetics and function. Unfortunately, the prevalence of impacted maxillary canines is about 1% to 3%; they are the second most common type of impaction after the third molars. In studies of maxillary canine impaction, white patients have shown frequencies of impaction in the palatal area that are twice those in the labial area. In contrast, Koreans have an incidence of impaction in the labial area that is 3 times that in the palatal area. Also, female patients show impaction twice as frequently as male patients do, and 8% have bilateral impactions of the maxillary canines.
Impacted canines can cause various problems such as cyst formation and root resorption of proximal teeth during eruption. Maxillary canine impaction is difficult to treat surgically or orthodontically, and the required treatment periods are long. Clinicians must carefully observe the eruption process for early diagnosis of maxillary canine impaction, eliminate local obstructing factors for proper eruption, or extract deciduous canines to prevent impaction. Therefore, for successful treatment of maxillary canine impaction, early diagnosis and careful observation are crucial.
Canine impaction can be diagnosed with visual examination, palpation, or radiography. In visual examinations, canine impactions are characterized by a delayed exfoliation of the deciduous canine, a difference in exfoliation times on the right and left sides, and an absence of permanent canine crown eminence about 10 years of age. In palpation examinations, canine gingival protuberance around 10 years of age is the key sign. In radiographic examinations, panoramic films. lateral cephalography, posteroanterior cephalography, and computed tomography are the diagnostic tools of choice. Recently, cone-beam computed tomography (CBCT) has become popular and provides many advantages for diagnosis of impacted teeth.
Proffit et al asserted that “In nearly every patient with malaligned teeth, the root apices are closer to the normal position than the crowns, because malalignment almost always develops as the eruption paths of teeth are deflected. Putting it another way, a tooth bud occasionally develops in the wrong place, but the root apices are likely to be reasonably close to their correct positions even though the crowns have been displaced as the teeth erupted.” Also, Scott reported that alignments of the dental lamina and the tooth germ are maintained in the form of catenary curves during the embryonic period. Thus, root apices of normally erupting, incompletely calcified teeth are expected to grow into normal arch forms. Canine impactions in the labial area show traits similar to those of the crowding form, and their root apices should also follow normal arch forms. However, palatally impacted canines appear to be developmental anomalies with genetic determinants, so their root apices should have an arch form different from normal ones. Unfortunately, there are no studies examining the relationship between root apex location and canine impaction. Three-dimensional (3D) images provided by CBCT can help with such studies. In this study, we used CBCT images to determine the coordinates of the root apices, which were then used to draw the corresponding arch forms.
The goals of this study were to determine the arch forms of root apices for normally erupting teeth and then determine the differences in apex location for impacted canines relative to normally erupting canines. In addition, we sought to determine whether the labiopalatal position of impacted canines influences the apex position.
Material and methods
This was a retrospective study. First, to identify the position of root apices for normally erupting canines, we included 21 patients with unerupted canines who subsequently had a normal history of permanent canine eruption and had CBCT images taken for another reason. The average age of this group was 8.5 ± 0.2 years (age range, 8.0-8.9 years; 11 girls, 10 boys). They were called the normal group. Second, to identify the position of root apices for impacted canines, we included patients with impacted canines who had CBCT images taken and were admitted to Pusan National University Dental Hospital. Unilateral impaction subjects were then selected to compare the impacted and nonimpacted sides. They were called the impaction group. The contralateral nonimpacted canine of the same patient was used as a control. The exclusion criteria were systemic disease, odontoma, mesiodens, or cleft lip and palate. Patients with low-resolution CBCT images or a small field of view for verification of root apex locations were also excluded. Each sample was classified according to the crown location of the impacted canine, specifically in the labiopalatal region, as the labial group, the palatal group, and the middle group. If the impacted canine crown touched the linear line between an adjacent lateral incisor and first premolar crown, we classified it into the middle group. The labial group included 27 patients (12 with 13 impacted teeth, 15 with 23 impacted teeth), the middle group included 17 patients (9 with 13 impacted teeth, 8 with 23 impacted teeth), and the palatal group included 21 patients (9 with 13 impacted teeth, 12 with 23 impacted teeth). The patients’ average age in these 3 groups was 13.1 ± 2.6 years (age range, 8.9-19 years; 34 girls, 31 boys).
This study was reviewed and approved by the institutional review board of Pusan National University Dental Hospital (number PNUDH-2013015).
A CBCT scanner (Pax-Zenith3D; Vatech Co., Seoul, Korea) was used to pinpoint the exact locations of the root apices. The CBCT settings were as follows: tube voltage, 90 kVp; scan time, 24 seconds; tube current, 4 mA; voxel size, 0.3 mm; and field of vision, 10 × 8 cm. CBCT data were converted and saved as DICOM files, and Ondemand3D (Cybermed Co., Seoul, Korea) was used to obtain the x, y, and z coordinates of the root apices.
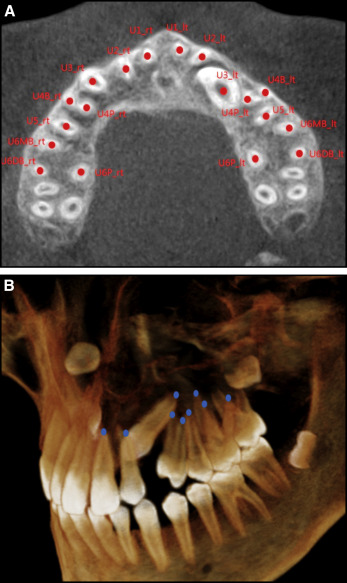
We defined nasion as the most anterior limit of the frontonasal suture on the frontal bone at the facial midline, and the CBCT scan was oriented horizontally with the palatal plane. We identified the palatal plane by 3 landmarks (anterior nasal spine and the center of greater palatine foramen on the right and left sides) in the multiplanar reformation mode of the Ondemand3D software. The relevant x, y, and z coordinates were obtained to locate the root apices of maxillary teeth, using nasion as the reference point origin (0, 0, 0) ( Fig 1 ). Even though the root apex was not fully calcified, the immature tips of the root were used as a landmark.
Two-dimensional coordinates were converted from acquired 3D coordinates via projection on a palatal plane. To process the converted 2-dimensional coordinates, the Procrustes function of the Matlab software (version 2014b; MathWorks, Natick, Mass) was used. Centroids and the sample size were translated and scaled, and then were rotated and superimposed. The Procrustes superimposition was also applied in the normal group, with the impaction group as the reference. For maxillary premolars or molars, the number of roots can vary from 2 to 3. In those cases, the root apex center was used as the landmark point.
Since the root apices’ arch forms showed a relatively symmetric distribution, the fourth-order polynomial function, excluding odd-power terms, was used for best curve fitting.
To measure the extent of root apex deviation from the root apices’ arch form, the average position of root apices was determined. Then, although distances for all other teeth were measured from their own average positions, the distances for impacted canines were measured from the average point for a contralateral nonimpacted canine, which was symmetrically moved to the opposite site.
Statistical analysis
One investigator (S.H.K.) recorded each measurement. To evaluate intraexaminer reliability, the data for 20 randomly selected impacted canines were reobtained. The second set of measurements was recorded at least 1 month after the first. The first and second sets of x, y, and z coordinate measurements were then subjected to a paired t test, which showed no statistically significant difference ( P >0.05). SPSS software (version 23.0; IBM, Armonk, NY) was used for the statistical analyses. An independent t test was used to determine the differences between the positions of unerupted canines in the normal group and contralateral nonimpacted canines in the impaction group, and the difference between the distances of the impacted canines to the average point and that of the contralateral nonimpacted canines. Also, a 1-way analysis of variance test was used to determine the differences between the 3 groups (palatal, middle, and labial). The Scheffé method was used for post hoc analysis, and the significance level was 5%.
Results
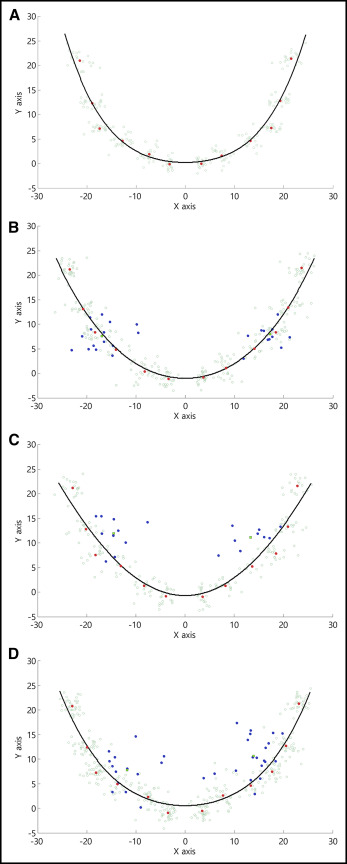
The root apices’ arch forms for each group are shown in Figure 2 . Despite immature calcification, the positions of normally erupting canines were aligned with normal root apices’ arch forms, whereas the impacted canines deviated from their root apices’ arch form. Also, the fourth-order polynomial functions, excluding odd-power terms for the root apices’ arch form, were calculated for the 4 groups. Each group’s distribution resulted in the following distinctive polynomial functions.
- 1.
Normal group: y = 0.2573 + 0.0192 x 2 + 4.0587 ×1 0 −5 x 4
- 2.
Palatal group: y = − 0.3555 + 0.0322 x 2 + 4.9587 × 10 − 6 x 4
- 3.
Middle group: y = − 0.3301 + 0.0312 x 2 + 6.3375 × 10 − 6 x 4
- 4.
Labial group: y = 0.6674 + 0.0209 x 2 + 2.6094 ×1 0 −5 x 4
The average x and y coordinates for the normal group were 13.16 ± 1.13 and 4.68 ± 1.31 from the origin; the average x and y coordinates for contralateral nonimpacted canines in the impaction group were 13.87 ± 2.07 and 5.17 ± 1.82. There were no statistically significant differences ( P >0.05).
For the impaction group, the average distances of each tooth from the root apices’ arch form are given in Table I . The contralateral, nonimpacted canines showed an average distance of 2.221 mm, and impacted canines were an average of 6.572 mm away, and the difference was statistically significant ( P = 0.000). The lateral incisors were farther away from the root apices’ arch form than the other normal teeth.


