Gingivitis
Plaque-induced Gingivitis, Gingivitis Simplex, Type I A 1
Gingivitis is ubiquitous. It is a bacterially-elicited inflammation (non-specific mixed infection) of the marginal gingiva (Löe et al. 1965).
In the chapter “Etiology and Pathogenesis,” the development and progression of gingivitis from healthy tissue to an early lesion and on to established gingivitis was described (pp. 56–59; Page & Schroeder 1976, Kornman et al. 1997). In children, the early lesion (gingivitis) with T-cell dominance can persist for many years; on the other hand, in adults, the persistent lesion is almost exclusively established gingivitis (with plasma cell dominance), which can assume quite variable clinical severity. It is possible, clinically and pathomorphologically, to differentiate gingivitis into mild, moderate and severe, although this classification is relatively subjective.
For a more precise diagnosis of gingival inflammation, it is prudent to employ accepted indices that quantitate bleeding upon probing of the gingival sulcus.

The borderline between healthy gingiva and gingivitis is difficult to ascertain. Gingiva that appears to be clinically healthy will nevertheless almost always exhibit histologically a mild inflammatory infiltrate. If there is an increase in clinical and histologic inflammation, one observes lateral proliferation of the junctional epithelium. The JE becomes detached from the tooth at its marginal aspect, as the bacterial front progresses between the tooth surface and the epithelium. The result is a gingival pocket.
In cases of severe gingivitis with edematous swelling and hyperplasia of the tissues, a clinical pseudopocket often forms.
Gingival pockets and pseudopockets are not true periodontal pockets because no connective tissue attachment loss has occurred, nor has there been apical proliferation of the junctional epithelium. However, because the milieu of pseudopockets is an oxygen-poor environment, periodontopathic anaerobic microorganisms can thrive.
It is true that gingivitis may develop into periodontitis. However, even without treatment, gingivitis can persist over many years in a stationary manner, exhibiting only minor variations in intensity (Listgarten et al. 1985). With treatment, gingivitis is fully reversible.
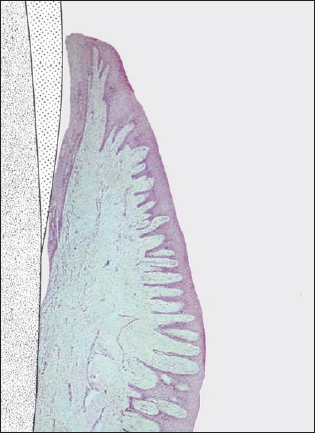
Histopathology
The clinical and histopathologic pictures of established gingivitis are well correlated (Engelberger et al. 1983).
The mild infiltration that occurs even in clinically healthy gingiva may be explained as a host response to the small amount of plaque that is present even in a clean dentition. Such plaque is composed of non-pathogenic or mildly pathogenic microorganisms, primarily gram-positive cocci and rods.
As plaque accumulation increases, so does the severity of clinically detectable inflammation, as evidenced by the quantity and expanse of inflammatory infiltrate. The subepithelial infiltrate consists primarily of differentiated Blymphocytes (plasma cells), with a smaller number of other types of leukocytes.
With increasing inflammation, more and more PMN granulocytes transmigrate the junctional epithelium. As a consequence, the junctional epithelium takes on the characteristics of a pocket epithelium (p. 104, Fig. 209; Müller-Glauser & Schroeder 1982), but without any significant apical proliferation.



Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


