Introduction
External apical root resorption (EARR) is a common complication in orthodontic treatment. Despite many studies on EARR, great controversies remain with regard to its risk factors. The objective of this study was to explore the relationship among sex, root movement, IL-1RN single nucleotide polymorphism (SNP) rs419598, IL-6 SNP rs1800796, and EARR associated with orthodontic treatment.
Methods
Altogether 174 patients (with 174 maxillary left central incisors) were selected for this study. Cone-beam computed tomography was performed before the start of the treatment and at the end of the treatment. Cone-beam computed tomography data were used to reconstruct a 3-dimensional image of each tooth; the volume and the root resorption volume of each tooth were calculated. Three-dimensional matching was used to measure the amount of movement of each root. Genomic DNA was extracted from buccal swabs, and genotypes of SNP rs419598 and SNP rs1800796 of each subject were determined using TaqMan polymerase chain reaction genotyping (Applied Biosystems, Foster City, Calif). The data were analyzed with multiple linear regression analysis.
Results
The statistical analysis indicated no relationship between sex, tooth movement amount, and IL-1RN SNP rs419598 with EARR. The IL-6 SNP rs1800796 GC was associated with EARR, and root resorption differed significantly between SNP rs1800796 GC and CC.
Conclusions
IL-6 SNP rs1800796 GC is a risk factor for EARR. The amount of root movement, IL-1RN SNP rs419598, and sex as risk factors for EARR need further study.
Highlights
- •
IL-6 SNP rs1800796 GC is a risk factor for external apical root resorption (EARR).
- •
Sex is not a risk factor for EARR.
- •
The amount of root movement for EARR needs further study.
- •
IL-1RN SNP rs419598 for EARR needs further study.
External apical root resorption (EARR) is a common complication in orthodontic treatment, and its possible risk factors include genetics, age, sex, and orthodontic treatment and duration.
After Newman reported in 1975 that EARR exhibits a familial aggregation, more studies have described the association of EARR with genetics. Al-Qawasmi et al showed that the IL-1beta (+3953/+3954) polymorphism in orthodontically treated subjects plays a role in the genetic influence on EARR and that the IL-1β allele 1 is a risk factor of EARR. Nevertheless, the case-control study of Gülden et al showed no difference between the alleles of IL-1beta. Iglesias-Linares et al also showed that the allele TT of IL-1RN single nucleotide polymorphism (SNP) rs419598 was highly and positively correlated with EARR. Although no correlation between IL-6 SNP and EARR has been reported up to now, studies have shown that the level of IL-6 in gingival crevicular fluid changes during orthodontic tooth movement, and the level of IL-6 is high in root resorption tissues. Therefore, as a multifunctional cytokine with both inflammatory and anti-inflammatory effects, IL-6 might play an important role in EARR.
Study results on the relationship between sex and EARR are controversial. Most studies showed no correlation, but some reported that the average amount of root resorption in female subjects is greater than that in male subjects.
Studies on the relationship between clinical factors and EARR are also complicated. Some studies have found that neither the size of the brackets nor the type of archwire is a risk factor for EARR, whereas sustaining force, tooth extraction treatment, overbite, Class II elastic pulling, and length of treatment are risk factors for EARR.
In most studies, the amount of root resorption was obtained using 2-dimensional x-ray films, such as periapical films, panoramic radiographs, and lateral cephalometrics. However, root resorption occurs 3 dimensionally and may occur at any site on the root. Katona and Yu et al also proved that neither periapical film nor panoramic radiograph was accurate enough for studying EARR clinically; this might also explain the discrepancies among the studies on EARR.
In recent years, cone-beam computed tomography (CBCT) has been used extensively in oral clinical work. Because CBCT can measure the width and length of the tooth at any 3-dimensional (3D) section accurately, studies on EARR with CBCT have demonstrated much improved accuracy and sensitivity. Wang et al proved that CBCT could accurately measure tooth and root resorption volumes and was a more accurate and reliable 3D measuring method for studying EARR.
Despite many studies on EARR, great controversies remain with regard to its risk factors, which may be attributed to 2 things: an inaccurate measuring method and the multifactorial nature of EARR. Therefore, in this study, we used a 3D volumetric measuring method to accurately measure the root resorption volume of the maxillary incisors and performed multiple linear regression analysis to explore the relationship among sex, root movement, IL-1RN SNP rs419598, IL-6 SNP rs1800796, and root resorption associated with orthodontic treatment.
Material and methods
This study was approved by the ethical board of Sichuan University in China. Participation was voluntary, and informed consent documents were signed by all participants before they entered this study.
The inclusion criteria were (1) patients treated with a straight archwire technique; (2) complete patients’ data before and after treatment, including sex, age before and after treatment, oral and facial photos before and after treatment, panoramic radiograph, lateral cephalometric, CBCT of the maxillary incisors, malocclusion type, therapy regimen, and so on; (3) the incisor crown undamaged during orthodontic treatment; and (4) finished development of the maxillary incisor. The exclusion criteria were (1) functional appliance used during treatment, (2) obvious root resorption of the maxillary incisors before treatment, (3) serious periodontitis, (4) abnormal root of the maxillary incisors, (5) developing maxillary incisor root, and (6) surgery needed.
Based on such criteria, 174 unrelated patients (68 male, 106 female; age range, 12-34 years), with 174 maxillary left central incisors, were selected for this study. All patients were from the Chinese Han population at the Department of Orthodontics, West China College of Stomatology, from 2009 to 2013, and every patient was treated with light forces. Treatment began with the thinnest nickel-titanium archwire with high elasticity, whose orthodontic force was very light, and the archwire was changed step by step as the tooth was aligned little by little. Severe crowding in the arch was aligned by stages to keep the forces light. A dynamometer was used to make sure that the force of elastic traction was light (<100 g). All treatments were completed in 14 to 28 months ( Table I ).
| Clinical and treatment variables | Mean (n) | SD (%) |
|---|---|---|
| Sex | ||
| Male | 68 | 39.1 |
| Female | 106 | 60.9 |
| Age (y) | 14.07 | 3.10 |
| Duration of treatment (mo) | 20.55 | 6.54 |
| Deep overjet | 86 | 49.43 |
| Anterior open bite | 29 | 16.67 |
| Extraction patients | 74 | 42.5 |
| Nonextraction patients | 100 | 57.5 |
| Angle classification | ||
| Class I | 75 | 43.10 |
| Class II | 89 | 51.15 |
| Class III | 10 | 5.75 |
The anterior maxilla was referred to CBCT scanning before and after treatment with the same CBCT machine (model MCT-1 [EX-2F]; J Morita, Kyoto, Japan) and the same parameters.
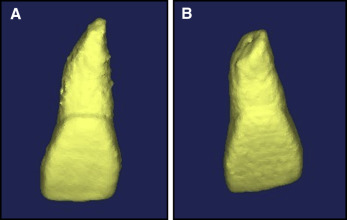
The CBCT data were collected in DICOM format. Mimics software (version 10.0; Materialise, Leuven, Belgium) was used for tissue segmentation, 3D reconstruction, and volumetric measurements. Root resorption volume during treatment was obtained by subtracting maxillary incisor volume after treatment from that before treatment ( Fig 1 ). Each tooth was measured 3 times, and the mean was used.
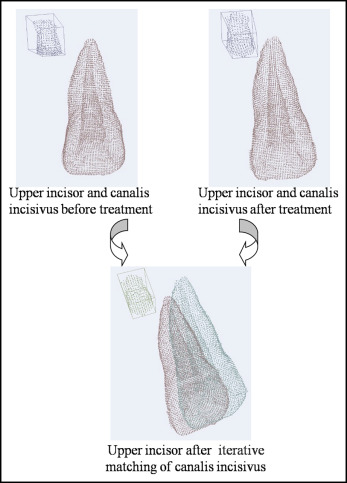
To measure the amount of movement of the maxillary incisor during treatment, the Mimics software was used to 3 dimensionally reconstruct the maxillary incisor and the canalis incisivus, and then the reconstruction was exported to the PLY format file. Iterative matching was used to match the canalis incisivus before and after treatment, and to transfer the canalis incisivus before and after treatment to the same coordinate system ( Fig 2 ). Then the maxillary incisors before and after treatment were matched to obtain the distance of translation and the angle of rotation. For each tooth, iterative matching was performed 3 times, and the best match was selected. The software for iterative matching was developed by the School of Life Science and Technology University of Electronic Science and Technology of China.
For DNA extracting and SNP genotyping, buccal cells were collected by scraping firmly against the inside of each cheek 10 times with a cotton swab when the orthodontic treatment was finished. DNA was isolated from the exfoliated buccal cells using an oral swab DNA extraction kit (BioTeke, Beijing, China) and stored with elution buffer at −80°C.
Real-time polymerase chain reaction was performed with the ABI 7900HT polymerase chain reaction instrument using TaqMan single nucleotide polymorphism assays (Applied Biosystems, Foster City, Calif) to complete the genotyping. The probe sequences designed by Applied Biosystems were rs419598: TATCTGAGGAACAACCAACTAGTTGC[C/T]GGATACTTGCAAGGACCAAATGTCA and rs1800796:ATGGCCAGGCAGTTCTACAACAGCC[C/G]CTCACAGGGAGAGCCAGAACACAGA. Each reaction mixture contained 12.5 mL of TaqMan universal polymerase chain reaction master mix, 0.65 mL of Taq-Man SNP kit (probe/primer mix), 4 mL of the DNA obtained, and 7.85 mL of DNase-free water in a final volume of 25 mL. Standard amplification conditions were 95°C for 10 minutes, 40 cycles of 92°C for 15 seconds, and 60°C for 40 seconds; 2 negative controls with sterile water as templates were used in each reaction plate. Allelic discrimination results were according to fluorescent signals from fluorescent dyes VIC and FAM (Applied Biosystems). The expected genotyping results were CT and TT for SNP rs419598, and CC and GC for SNP rs1800796.
Statistical analysis
Male subjects were assigned number 0, and female subjects were assigned number 1; CT genotype of IL-1RN SNP rs419598 was assigned number 0, and TT was assigned number 1; CC genotype of IL-6 SNP rs1800796 was assigned 0, and CG was assigned 1.
Tooth movement includes translation (millimeters) and rotation (degrees), and rotation consists of the 3 directions of x, y, and z, and thus the sum of 3 axial rotation angles was obtained.
The data base was established with Excel software (version 2010; Microsoft, Redmond, Wash), and the relationship among sex, amount of root translation, amount of root rotation, IL-1RN SNP rs419598, IL-6 SNP rs1800796, and root resorption volume was analyzed using multiple linear regression analysis. The regression model hypothesis test was performed with software (version 16.0; SPSS, Chicago, Ill) to get the multiple linear regression equation: yˆ = b 0 + b 1 ·X 1 + b 2 ·X 2 + … + b m ·X m , P <0.05 was considered statistically significant. The Bonferroni adjustment was used to control type I error. Power analysis was performed with PASS 11 software (NCSS, Kaysville, Utah).
Results
The frequencies of rs1800796 genotypes were 108 CC and 66 GC. The frequencies of rs419598 genotypes were 30 CT and 144 TT. In these 174 maxillary left central incisors, the root resorption volumes ranged from 0 to 32.97 mm 3 , with a mean volume of 12.59 ± 6.27 mm 3 ( Table II ).
| Genotypes | Frequency | Root resorption volume | |
|---|---|---|---|
| rs1800796 | CC (108) | GC (66) | |
| rs419598 | CT (30) | TT (144) | Maximum, 32.97 mm 3 Mean, 12.59 ± 6.27 mm 3 |
The independent sample t test showed that sex did not differ significantly ( Table III ); neither did the genotypes of IL1ra SNP rs419598 ( Table IV ). IL-6 SNP rs1800796 CC and GC genotypes differed significantly ( Table V ).
| Root resorption | ||||
|---|---|---|---|---|
| n | Mean | SD | ||
| Sex | Male | 68 | 11.73 | 6.62 |
| Female | 106 | 13.14 | 6.00 | |
| F | 1.61 | |||
| P | 0.15 | |||
| Root resorption | Root resorption | |||
|---|---|---|---|---|
| SNP | n | Mean | SD | |
| CT | 30 | 10.99 | 6.00 | |
| TT | 144 | 12.92 | 6.29 | |
| F | 0.09 | |||
| P | 0.13 | |||
| Root resorption | ||||
|---|---|---|---|---|
| SNP | n | Mean | SD | |
| CC | 108 | 11.50 | 6.02 | |
| GC | 66 | 14.38 | 6.30 | |
| F | 0.35 | |||
| P | 0.003 | |||
According to the result of single-factor analysis, sex and genotypes of IL1ra SNP rs419598 were excluded from the variances of multiple linear regression analysis. The result of the regression model hypothesis test was F=SSR/SSE=3.54
F = SSR / SSE = 3.54
( P <0.05), indicating that the regression model had statistical significance ( Table VI ).


