and Paolo Biondi2
(1)
Aesthetic and Maxillofacial Surgery, Padova, Italy
(2)
Maxillofacial Surgery, Forlì, Italy
Abstract
Looking at the upper third of the face, we can note its role in facial expression. The acts of blinking, raising or lowering the eyebrows, frowning the glabella, elevating the upper lids, closing the eyes, and rotating the eye globes up or down are essential in communicating approval or disapproval, attention, surprise, indifference, and many other emotions. In the long term, the aging process progressively changes the external aspect of the upper third, as well as its dynamics.
Looking at the upper third of the face, we can note its role in facial expression. The acts of blinking, raising or lowering the eyebrows, frowning the glabella, elevating the upper lids, closing the eyes, and rotating the eye globes up or down are essential in communicating approval or disapproval, attention, surprise, indifference, and many other emotions. In the long term, the aging process progressively changes the external aspect of the upper third, as well as its dynamics.
For these reasons, the analysis of the upper third of the face is not limited to a simple three-dimensional assessment of symmetry, proportion, and shape of the region, but must include the fourth dimension of dynamics and the fifth dimension represented by the effects of the aging process.
6.1 Forehead Analysis
The forehead occupies the upper third of the face entirely, and its bony shape and muscle activity are intimately associated with the aesthetics and functions of the orbital and nasal units; its width is about twice its height.
Two skeletal subunits can be considered: the supraorbital bar and the upper forehead [5]. The supraorbital bar, corresponding to the supraorbital rim and glabellar area, greatly influences the aesthetics of the brow, the upper lid, and the nasal radix, due to its direct structural support. Its shape varies widely with the development of the frontal sinus, with more angularity and anterior prominence in male subjects than in female ones.
The upper forehead, located above the supraorbital bar, consists of a slight vertical and transversal convexity. The palpable and often visible rim of the temporal fossa, also called the temporal ridge, is the lateral boundary of the forehead. The hairline, which defines the forehead upper boundary, is quite different between the sexes and, especially in relationship with men’s anterior balding, can change with age.
When analyzing the bony forehead, three important aesthetic characteristics should be considered: the general shape, the slope, and the morphology of the supraorbital bar. The outline, in profile and oblique views, varies from round to flat with, sometimes, an inferior concavity defining the supraorbital ridge. The basal view is useful in defining the symmetry and the grade of transversal convexity.
The soft tissue analysis of the forehead should recognize the glabellar frown lines and the transverse forehead wrinkles or furrows along with the evaluation of the regional muscle dynamics.
Even if the forehead can be reshaped surgically with specific procedures, in the vast majority of cases, it should be considered as a stable and highly visible skeletal structure that can be utilized as a reference in the process of analysis of the shape, volume, and spatial orientation of other structures such as the nose, the midface, the anterior teeth, and the chin.
The temporal region, which is bounded inferiorly by the zygomatic arch, anteriorly by the posterior rim of the frontal process of the malar bone and the zygomatic process of the frontal bone, and superiorly by the rim of the temporal fossa, can vary from slightly concave to slightly convex depending on the volume of temporal muscle and subcutaneous fat. The shape and location of the temporal hairline have an important role as a boundary in the aesthetics of the upper third of the face.
6.2 Eyebrow, Eye, and Lids Analysis
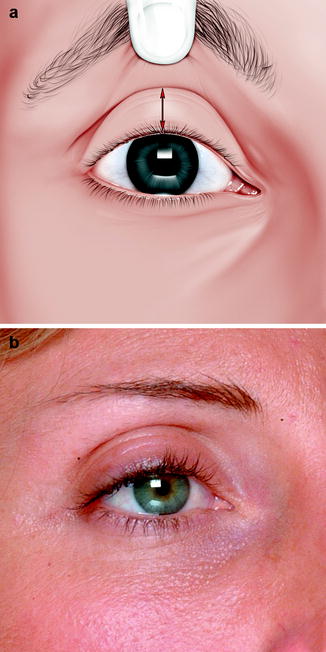
From the aesthetic and functional point of view, there is no sense in evaluating the eyebrow separately from the upper lid or any other component of the orbital region. Figure 6.1 shows the surface anatomy of the orbital region along with the related basic terminology.
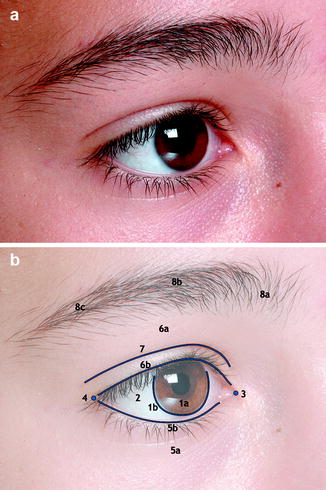
Fig. 6.1
Close-up oblique view of orbital region in a young subject (a). Basic elements of normal surface anatomy of the orbital region (b): 1a iris, 1b limbus (the circular line separating the iris from the white sclera), 2 white sclera, 3 medial canthus, 4 lateral canthus, 5a lower lid, 5b lower lid free margin, 6a upper lid, 6b upper lid free margin, 7 upper lid crease, 8a medial third of the eyebrow (head), 8b central third of the eyebrow (body), and 8c lateral third of the eyebrow (tail)
The assessment of the skeletal support sustained by the orbital ridges and the globe to soft tissue requires the visualization in profile view of three different vertical reference lines, which, in the frontal view, pass through the center of the iris (Fig. 6.2a):
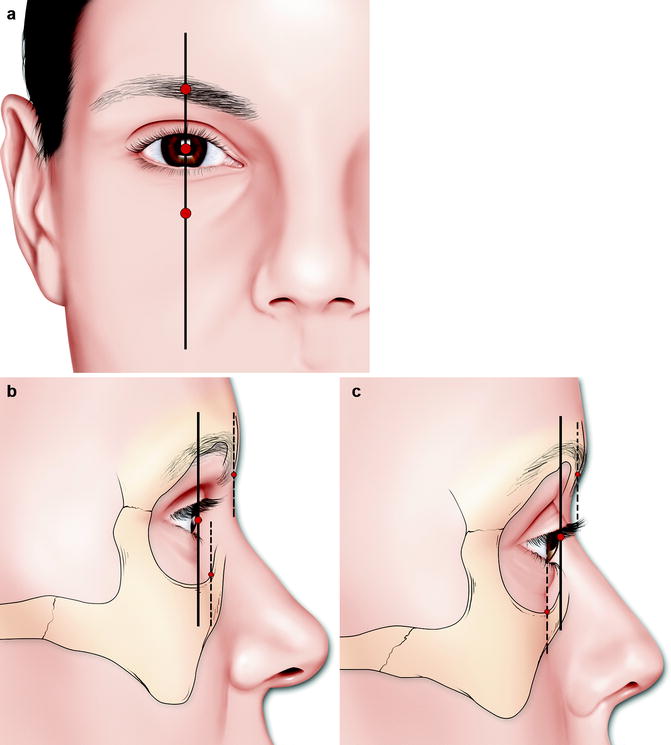
Fig. 6.2
The corneal plane line, the upper orbital rim line, and the lower orbital line coincide in the frontal view (a). In the case of a normally positioned eye globe, the upper orbital rim line lies anterior to the corneal plane line, whereas the lower orbital rim line can be anterior (b) or posterior (c) to it
-
The corneal line. This is the reference line and requires that the eye globe be in a normal sagittal position.
-
The upper orbital rim line. This is 8–10 mm anterior to the corneal plane line depending on the pneumatization of the frontal sinus and the morphology of the supraorbital bar [6].
-
The lower orbital rim line. Its position can vary widely from posterior to anterior with respect to the corneal plane line. A protrusive lower orbital rim is associated with good lower lid support and a youthful aspect (Fig. 6.2b), whereas a recessive lower orbital rim line is a sign of infraorbital and midface hypoplasia, which is associated with inadequate support of the lower lid and poor aesthetics (Fig. 6.2c).
The oblique views, examining the upper portion of the ogee curve,1 are also extremely useful in the evaluation of the skeletal support offered to the lower lid by the inferior and lateral traits of the orbital rim.
6.2.1 The Female Attractive Eye
Many authors have studied the attractive female eye and brow, producing the criteria that were assembled and reformulated by Gunter and Antrobus in their article of 1997 [3]. Some of these are:
-
Eyebrow shape.2 This forms a gentle curve without angularity (Fig. 6.3a). The medial and central portions are wider than the lateral portion (Fig. 6.3b).
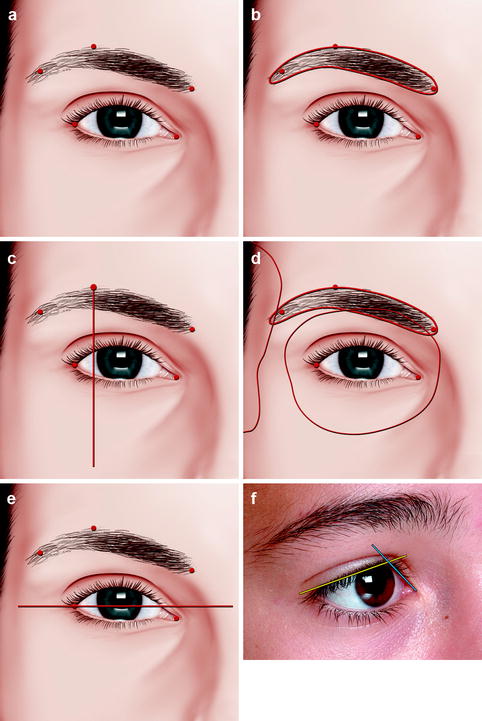 Fig. 6.3The female attractive eye. The eyebrow shape forms a gentle curve without angularity or interruptions (a); the medial and central portions are wider than the lateral (b). The eyebrow peak is located on a vertical plane passing lateral to or touching the lateral limbus (c). The medial third of the brow lies on the orbital ridge or partially inferior to it, the central third is on the ridge, and the lateral third just above the ridge (d). The intercanthal axis should be inclined slightly upward from medial to lateral, producing an upward lateral canthal tilt (e). The medial portion of the upper lid margin should be more vertically oriented than the lateral one (f)
Fig. 6.3The female attractive eye. The eyebrow shape forms a gentle curve without angularity or interruptions (a); the medial and central portions are wider than the lateral (b). The eyebrow peak is located on a vertical plane passing lateral to or touching the lateral limbus (c). The medial third of the brow lies on the orbital ridge or partially inferior to it, the central third is on the ridge, and the lateral third just above the ridge (d). The intercanthal axis should be inclined slightly upward from medial to lateral, producing an upward lateral canthal tilt (e). The medial portion of the upper lid margin should be more vertically oriented than the lateral one (f) -
Eyebrow peak. This is located on a vertical plane passing slightly lateral to or touching the lateral limbus (Fig. 6.3c).
-
Eyebrow location. The medial end of the eyebrow starts on the same or near the vertical plane of the medial canthus if there is a normal intercanthal distance. The medial third lies on the orbital ridge or partially inferior to it, the central third is on the ridge, and the lateral third just above the ridge (Fig. 6.3d).
-
Intercanthal axis. It should be inclined slightly upward from medial to lateral, producing an upward lateral canthal tilt (Fig. 6.3e).
-
Upper lid–iris relationship. The upper lid should cover the iris by approximately 1–2 mm.
-
Medial and lateral portions of the upper lids margin. The medial portion should be more vertically oriented than the lateral one (Fig. 6.3f).
-
Upper lid crease. It should parallel the lash line and divide the upper lid into an upper two thirds and a lower one third.
-
Medial and lateral extension of the upper lid crease. The medial extension should not exceed the inner extent of the medial canthus, and the lateral one should not extend beyond the lateral orbital rim.
-
Lower lid–iris relationship. There should be minimal, if any, scleral show between the lower lid and iris.3
-
Lower lid margin. It should bow gently from medially to laterally, with the lowest point between the pupil and the lateral limbus.
The main differences in the attractive male eye are in the intercanthal axis, which is less inclined upward from medial to lateral, in the supraorbital ridge anterior projection, which is augmented, and in the brow, which is wider, less arched, and more horizontally oriented. Figure 6.4 shows a comparison between an attractive female and an attractive male eye.
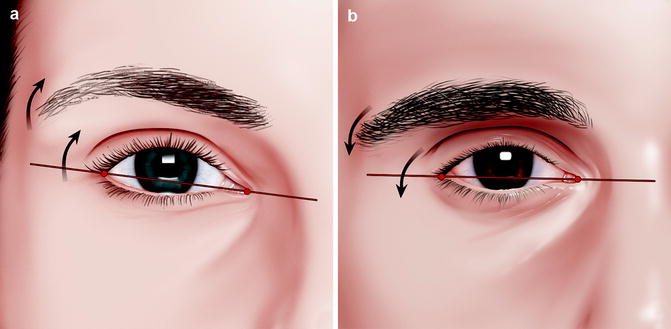
Fig. 6.4
Comparison between the female attractive (a) and the male attractive eye (b). In male subjects, the intercanthal axis is less inclined upward from medial to lateral, the supraorbital ridge anterior projection is augmented, and the brow is wider, less arched, and more horizontally oriented
6.3 Upper Lid Crease Malposition
The vertical position of the upper lid crease must be assessed with precision during clinical examination. It may be related to different conditions such as ethnicity, aging, and levator muscle dehiscence from the tarsal plate [8].
To evaluate the vertical position of the upper lid crease precisely, we can utilize the margin crease distance. It is the distance from the central upper eyelid margin to the tarsal crease measured with the eyelid fold elevated by the examiner and as the patient looks down (Fig. 6.5a). The normal range in occidentals reported by Putterman is 9–11 mm [7], whereas that reported by Wolfort, Baker, and Kanter is 8–10 mm [9].
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


